|
Abstract
Frailty is a common, heterogeneous, geriatric
syndrome associated with adverse health events.
There is a lack of knowledge concerning the relationship
between two multidimensional variables: frailty
and quality of life (QOL).
Aim: was to investigate the relationship
between frailty and health-related quality of
life (HR-QOL) among community dwelling non demented
elderly.
Method: 115 non demented elderly, 60 years
and older recruited from outpatient geriatric
clinic at Al Mansoura General Hospital, Dakahlia,
Egypt. Each participant underwent Comprehensive
geriatric assessment, assessing the health related
Quality of life (HR-QOL) by the RAND-36 health
survey and assessing frailty by Edmonton frail
scale (EFS).
Results: Frailty significantly correlates
with all the 8 dimensions of the HR-QOL even after
controlling for covariates. Also frailty status
significantly correlates with age, education,
Body Mass Index (BMI), function, depression and
cognition. By linear Correlation coefficient a
significant correlation between frailty and HR-QOL,
age, function, cognition and depression was found.
Conclusion: Dimensions of HR-QOL were negatively
affected by frailty and that possible correlates
of frailty status were age, low socioeconomic
status, low body mass index, functional dependence,
depression and cognitive impairment. Effort to
improve quality of life for frail elders in this
population is important.
Key words: Community dwelling elderly,
Frailty, Quality of life.
|
- - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
Introduction
Aging involves progressive decline in the functional
reserve of multiple organs and systems due to limitation
in functional reserve, damage from environmental agents,
increased prevalence of chronic diseases and the emergence
of a number of conditions termed geriatric syndrome
(1). One of these syndromes is Frailty. It is a syndrome
of decreased reserve and resistance to stressors, resulting
from cumulative declines across multiple physiologic
systems, causing vulnerability to adverse health outcomes
including falls, hospitalization, institutionalization
and mortality (2-8). The frailty phenotype model(4)
has been defined as any three of weight loss, self-reported
exhaustion, low activity levels, low walking speed and
low grip strength.
Frailty is multidimensional, heterogeneous and unstable,
thus distinguishing it from disability or ageing alone
(9). Rather, it is widely conceived of as a state of
vulnerability. Frailty is measured in many ways, including
'rules based' instruments, summative impairment lists
and algorithms derived from clinical judgment (10-12).
Frailty is highly prevalent in older people; up to 40%
of older people can be considered as frail and an increasing
trend can be expected (13). Next to its high prevalence,
frailty is characterized by its seriousness as it is
related to an increased risk of adverse health outcomes
such as disability (14), functional decline, hospitalization
and death (15,16). These poor outcomes, in turn, can
have negative implications on health related quality
of life (HRQOL) (17-19).
HR-QOL is defined as: "The value assigned to the
duration of life as modified by the impairments, functional
states, perceptions and social opportunities that are
influenced by disease, injury, treatment or policy (20)
HR-QOL, however, it involves more than a self-assessment
of functional status; it also conveys an individual's
sense of satisfaction with that level of functioning"
(21).
Only very few randomized controlled trials targeting
frail older people have considered QOL among outcomes
(22).
Until now, research on frailty has largely ignored the
effect of frailty on psychosocial outcomes such as health
related quality of life. In order to explore the extent
to which frailty permeates a person's life, we examined
the relationship between frailty and health related
quality of life in a sample of older Egyptians.
As intervention in the early stages of frailty may lead
to reversal of the syndrome and minimize if not prevent
some of its associated adverse outcomes (23), so interventions
to prevent, delay, or reverse frailty may have a beneficial
impact on the health related quality of life in the
elderly.
The current study examines the relationship between
frailty and HR-QOL in community dwelling non demented
elderly, while accounting for other domains of clinical
importance such as cognition, functional limitation
and depression.
Subjects and Method
Study population was 115
non demented elderly patients 60 years and above recruited
from the outpatient geriatric clinic at Al Mansoura
General Hospital, Egypt, both males and females, with
consent to participate and able to answer the questionnaire
during the interview.
Participation was based on informed consent from all
participants and the study was approved by the scientific
board of Geriatrics and Gerontology department, Faculty
of Medicine, Ain Shams University.
Each participant was assessed by an experienced clinician
and underwent Comprehensive Geriatric Assessment (CGA)
in the form of;
a) Detailed medical history, and clinical
examination.
b) Assessment of cognitive function using the
1) Mini Mental state Examination (MMSE) (24).
The MMSE is a brief 30-point questionnaire test that
is used to screen for cognitive impairment. It is commonly
used in medicine to screen for dementia. The MMSE examines
orientation, immediate and short-term memory, attention
and calculation, language and praxis. An Arabic version
was used (25).
Age, education, cultural and socioeconomic background
can cause a considerable bias in the MMSE's scores (26),
so results were correlated with the age and educational
level of the participants.
c) Screening for depression by Geriatric
depression scale 15 items (27), using an Arabic version
(28).
d) Functional assessment
By Activities of Daily Living (ADL) (personal care,
clothing, moving, going to the toilet, eating) were
measured with the Katz scale (29). The total score ranges
from 0 to 6 with higher scores meaning better function
(29) . The Lawton's assessment scale was used to assess
abilities in Instrumental Activities of Daily Living
(IADL), such as making phone calls, shopping, driving
and using money (30). The scores range from 0 to 8 with
higher scores meaning better function (30).
e) Assessment
of Health Related Quality of Life (HR-QOL)
HR-QOL is measured with the RAND-36 Arabic version (31).
The tool includes the same items as those in the SF-36
and the MOS-36 (32). It is a frequently used instrument
in the research of HR-QOL in relation to aging (33).
The RAND- 36 measures the perception of health on eight
dimensions: physical functioning, social functioning,
role limitations due to physical problems, role limitations
due to emotional problems, emotional well-being, energy/fatigue,
bodily pain and general health perception. The scores
are converted to a 0 to 100 scale, with higher scores
indicating higher levels of well-being or functioning
(31).
The RAND-36 has proven to have a good validity (31).
f) Assessment of frailty by the Edmonton Frail Scale
(EFS),
The EFS (34) samples 10 domains; Two domains are tested
using performance-based items: the Clock test (35) for
cognitive impairment and the 'Timed Get Up and Go' (36)
for balance and mobility. The other domains are mood,
functional independence, medication use, social support,
nutrition, health attitudes, continence, burden of medical
illness and quality of life (all standard historical
items in geriatric assessment). The maximum score is
17 and represents the highest level of frailty, on a
proposed five-level categorization (robust = 0-4, apparently
vulnerable (pre-frail) = 5-6, mildly frail = 7-8, moderately
frail = 9-10, severely frail = 11-17 (34).
The EFS correlated significantly
(r= 0.64, p<0.001) with the Geriatrician's clinical
impression of frailty (based on a 1 hour CGA) and medication
count (r= 0.34, p<0.001) (34).
A unique characteristic of the EFS as a clinical frailty
instrument is its inclusion of the domain of social
support, suggesting an endorsement of the dynamic model
of frailty (37).
g) Assessment of body mass index (BMI):
We classified subjects as regards to BMI according to
National Institutes of Health guidelines regarding body
size classification (38). Body mass index (BMI) categories
(underweight, normal weight, overweight, or obese)
The following subjects were excluded from the study:
- Those with severe cognitive impairment as detected
by MMSE <10 = severe impairment (39).
- Those with either severe hearing, visual and functional
impairments preventing them from completing the questionnaires.
There have been reports about the adverse effects of
age, severe cognitive impairment and physical status
on rates of self-completion of the SF-36 (40-42).
All the questionnaires were done with face-to-face interview
with each participant, as high illiteracy level was
present between the participants and to avoid the problems
associated with self-completion.
Statistical analyses
Statistical presentation and analysis of the present
study was conducted, using the chi-square for qualitative
data and T- test and ANOVA for quantitative data and
Linear Correlation Coefficient; also ANCOVA for analysis
of co variants by SPSS V18.
Results
Among the 115 non-demented
participants, 74.78% (n=86) were 60 to 74 years old,
25.22% (n=29) were 74 to 85 years, mean age was 67.452
± 5.382, 37.39% (n=43) were males and 62.61%
(n=72) were females. The majority of the participants
were illiterate 59.13% (n=68), 29.57% (n=34) can read
and write and only 2.61(n=3) had primary education,
7.83% (n=9) had secondary education and 0.87% (n=1)
had high education.
According to EFS, robust represented 44.35% ( n=51),
pre frail was 20.87% (n=24), while mild frailty represented
15.65% (n=18), moderate frailty was 13.91% (n= 16) and
severe frailty was 5.22% (n=6) of the studied sample.
Table 1 presents baseline characteristics of the participants
stratified by frailty status.
Click here for Table 1: Characteristics
of participants according to Edmonton frail scale (EFS)
by number and % (n (%)
Regarding demographic data and past medical history,
it was found that the frail group were older, had greater
prevalence of stroke, widowhood and had lower education
than the non frail group.
Regarding MMSE, ADL and IADL those who were frail had
lower scores than the non-frail and pre-frail participants,
and the increase in the level of frailty was associated
with worse scores in MMSE, ADL and IADL, that is to
say that the severely frail had lower scores than those
with moderate and mild frailty. (Table 2)
Click here for Table 2: Characteristics
of participants according to Edmonton frail scale (EFS)(
by Mean and SD) (M ± SD)
Regarding GDS, those who were frail had lower scores
than the non-frail and pre-frail participants and the
highest GDS scores were found in the severe frailty
group compared to the moderate and mild frailty groups.
(Table 2)
The same pattern was found for HR-QOL scores on the
RAND-36 scales, in that those who were frail had lower
scores than the non-frail and pre-frail participants,
and the worst scores were found in the severe frailty
group compared to the moderate and mild frailty groups.
(Table 2)
Regarding BMI, it was found that the frail groups (mild,
moderate and severe) were significantly more underweight
than the robust group. (Table 1)
We wanted to determine the true correlation between
frailty and HR-QOL, therefore we performed multiple
regression analyses by analysis of co-variants (ANCOVA)
controlling for confounders (age, ADL, IADL, GDS, MMSE
and education) and we found that still there is a significant
correlation between RAND-36, assessing HR-QOL, and frailty
assessed by EFS (Table 3)
Table 3: Correlation between RAND-36 and Edmonton
frail scale after adjustment for age, education, MMSE,
ADL, IADL and GDS.
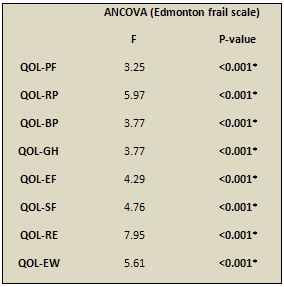
QOL= quality of life,PF= Physical functioning, RP=Role
limitation-physical, BP= Bodily Pain, GH= General health,
EF= Energy/fatigue, SF=Social functioning, RE=Role limitation-emotional,
MH= Mental health
By Linear Correlation Coefficient, there was a negative
significant correlation between EFS and all the 8 RAND-36
subscales (assessing HR-QOL), ADL, IADL and MMSE while
there was a positive significant correlation between
EFS and age and GDS.(Table 4).
Table 4: Linear Correlation Coefficient between EFS
scores and different variables:
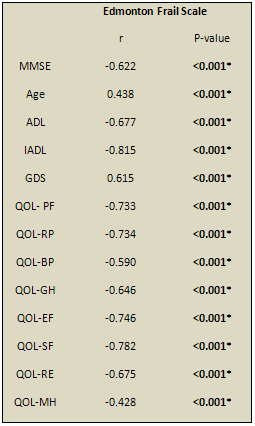
QOL= quality of life, PF= Physical functioning, RP=Role
limitation-physical, BP= Bodily Pain, GH= General health,
EF= Energy/fatigue, SF=Social functioning, RE=Role limitation-emotional,EW=emotional
well-being, MMSE= mini mental state examination, GDS=
geriatric depression scale, ADL= activities of daily
living, IADL= instrumental activities of daily living
BMI significantly correlates to Edmonton frail scale
scores. Underweight elderly show higher EFS scores than
normal weight elderly as shown in Table 5.
Table 5: Correlation between Edmonton frail scale
and BMI
 BMI
= Body mass index BMI
= Body mass index
P-values were calculated by ANOVA test.
Significant P-value (<0.05)
Discussion
In this cross-sectional study of the complex relationship
between frailty status and HR-QOL in a sample of community-dwelling
non demented older outpatients, we used two recently
validated assessment tools: the EFS to assess frailty,
it has five-level categorization of the frailty status
from robust to pre-fail to mild to moderate to severe
frailty, and this categorization is not found in most
frailty scales as reported by Rolfson et al (34), and
the RAND-36 health survey to assess HR-QOL. It is a
frequently used instrument in the research of HR-QOL
in relation to aging, Hickey et al (43).
The correlation between frailty and QOL; our
results indicate that frail subjects (mild, moderate
and severe frailty) had significantly poorer HR- QOL
eight dimensions which are physical functioning, bodily
pain, role limitations due to physical health problems,
role limitations due to personal or emotional problems,
emotional well-being, social functioning, energy/fatigue,
and general health perceptions, comparable to robust
and pre-frail elderly even after controlling for possible
confounders such as age, functional dependence, education,
cognition and depression. Also by Linear Correlation
Coefficient there was a significant negative correlation
between EFS scores, assessing frailty, and all RAND-36
subscale scores, assessing HR-QOL. These results were
consistent with other studies that found that frail
subjects reported a worse overall QOL than pre-frail
and non-frail subjects as detected by Fried et al(4),
Eklund & Wilhelmson (22), Ravaglia et al (45), Avila-Funes
et al (46), Masel et al (47), and Kanauchi et al (48)
. A study done by Puts et al (49), reported that among
a smaller group (n=25) of community-dwelling older adults,
those who were frail reported worse health-related quality
of life than those who were non-frail. The authors suggested
that a larger study could confirm the findings.
On the other hand, Bilotta et al (50), found that frail
subjects reported a worse overall QOL using old people
quality of life (OPQOL), than pre-frail and non-frail
subjects. They found that, five of the seven dimensions
of QOL were found to be impaired in frail older participants
which are health, independence, home and neighborhood,
psychological and emotional well-being, and leisure,
activities and religion, only the QOL domains of "social
relationships and participation" and "financial
circumstances" were not significantly different
among the three "frailty status" groups. In
our study QOL was assessed by RAND-36 which is a health
related QOL questionnaire, while their study assessed
QOL by OPQOL which assesses other domains of QOL as
psychological well-being, home and neighborhood, and
leisure activities and religion, which are the social
context of QOL. There is a difference between QOL and
health related quality of life (HR-QOL). Because QOL
has a highly individualistic, subjective and multidimensional
nature, it is difficult to define and measure as mentioned
by Guse & Masesar (51). Therefore HR-QOL is used
more regularly in research, Smith et al (52). But it
is important to assess all domains of QOL and their
correlation to frailty.
On the other hand some studies failed to find a strong
correlation between frailty and QOL, such as a study
by Andrew et al (53) on community dwelling elderly,
where a social vulnerability index for living situation,
language, social support, social and leisure activities,
relationships, and socio-economic status was weakly
correlated with a frailty index created by Rockwood
& Mitnitski (15).
We can say that frailty, even mild degrees, has a negative
effect on health related QOL, but the difference between
studies can be due to the difference of the tests and
scales used to assess QOL. Other differences might be
the participants, either community dwelling elderly,
or elderly in elderly caring facilities, along with
the sample size. So, further studies are needed with
a larger sample size and using scales assessing all
the domains of QOL to assess the correlation of frailty
to QOL.
Frailty
and its correlates: Prevalence of frailty among
the studied group as assessed by Edmonton frail scale
was mild frailty which represented 15.65% (n=18), moderate
frailty was 13.91% (n= 16) and severe frailty was 5.22%
(n=6) of the studied sample, that is to say about 34.8%
had frailty status.
This high prevalence agrees with a cross-sectional study
by Billota (50) where according to the Study of Osteoporotic
Fractures (SOF) criteria (30%) were "robust",
(37%) were "pre frail" and (33%) were "frail".
While in another study by Fried et al (4), in which
frailty was defined as the presence of three out of
five criteria; shrinking/weight loss, weakness, poor
endurance and energy, slowness and low physical activity,
found a prevalence of 7% in men and women aged 65 years
and older.
This high prevalence in frailty status found in our
study can be explained by that our participants are
outpatients; it was found that frail subjects make larger
use of health and community services than subjects who
are not frail, as shown by Rochat et al (54). Also the
low socioeconomic status of the participants, as there
is a high prevalence of illiteracy, has been associated
with frailty in several cross-sectional studies such
as Blaum et al (55), Newman et al (56), Burke et al
(57) and Fried et al (58).
It
was found that those who were frail were older, had
lower education, had more prevalence of stroke, were
more functionally dependent in ADL and IADL, had more
depressive symptoms by GDS and had more cognitive impairment
by MMSE, and the degree of frailty had an inverse relation
to function, cognition, and a positive relation with
age and depression. This was also found by Linear Correlation
Coefficient that showed a significant negative correlation
between the EFS scores and ADL, IADL, and MMSE scores
and a positive correlation between EFS scores and age
and GDS scores. Regarding age, Woods et al (59), found
that increased chronological age has been associated
with frailty, even after adjustment for medical co morbidities.
Regarding prevalence of stroke, it was found to be a
risk factor to frailty as detected by Woods et al (59)
, while regarding cognition, Central nervous system
(CNS) function and cognitive impairment have been hypothesized
to be either components of frailty or risk factors as
reported by Studenski et al (60). Regarding function,
it was found that frailty is predictive of disability,
as baseline frailty was strongly associated with ADL
disability at 3- year follow-up study by Woods et al
(59), while regarding depression, depressive symptoms
have been shown to be associated with the frailty syndrome
in cross-sectional analyses by Fried et al (4). Another
found a strong prospective relationship between depressive
symptoms and the onset of frailty, suggesting that depression
may contribute to the etiology of frailty as described
by Woods et al (59). Further studies are recommended
designed to assess correlates of frailty status, to
support our findings.
Regarding BMI, it significantly correlates to the Edmonton
frail scale, as about (87%, n=20) of the underweight
elderly (n=23) were frail. Underweight elderly show
higher EFS scores than normal weight elderly. Weight
loss is one of the components of the frailty model proposed
by Fried et al (4) and inadequate nutrition is commonly
recognized clinically as a marker of frailty. Subjects
in the Cardiovascular Health Study (CHS) by Walston
et al (61) categorized as frail included both a subset
who were underweight and a subset with higher body mass
index (BMI) consistent with obesity.
Previous research has shown that frailty is a dynamic
state that is responsive to focused interventions as
found by Fried et al (23) and Newman et al (62), so,
it may be possible to modify some of the factors associated
with frailty, including socioeconomic status, strength
and exercise tolerance, psychological wellbeing, cognition
as well as comorbid illness and disability, and this
may have desirable effects on perceived HRQOL. Further
studies are needed to support this.
Study limitations included the small sample, only out
patients, as well as the cross-sectional approach of
our analyses, which is mainly due to lack of cooperation
of elderly as the concept of doing scientific research
is still not widespread in our community, which decreases
the generalization of the current findings.
Conclusion
We can conclude that being frail was strongly associated
with diminished health related quality of life. Possible
correlates of frailty status were age, low socioeconomic
status, low body mass index, functional dependence,
depression and cognitive impairment.
Interventions to prevent, delay, or reverse frailty
may have a beneficial impact on the health related quality
of life in the elderly.
List of abbreviations
ADL = activities of daily living, BMI= body mass
index,
EFS = Edmonton frail scale,
GDS = geriatric depression scale,
HRQOL = health related quality of life,
IADL = instrumental activities of daily living,
MMSE = mini mental state examination.
References
1) Kinney JM . Nutritional frailty, sarcopenia and falls
in the elderly. Curr Opin Nutr Metab Care 2004;7:15-20.
2) Bauer JM, Sieber CC. Sarcopenia and frailty: a clinician's
controversial point of view. Exp Gerontol 2008;43(7):674-678
3) Bandeen-Roche K, Xue QL, Ferrucci L, Walston J, Guralnik
JM, Chaves P, Zeger SL, Fried LP. Phenotype of frailty:
characterization in the women's health and aging studies.
J Gerontol A Biol Sci Med Sci 2006; 61 : 262-266
4) Fried LP, Tangen
CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman
T, Tracy R, Kop WJ, Burke G, McBurnie MA; Frailty in
older adults: evidence for a phenotype. J Gerontol A
Biol Sci Med Sci 2001;6 : 146-56
5) Gill TM, Gahbauer
EA, Allore HG, Han L. Transitions between frailty states
among community-living older persons. Arch Intern Med
2006; 166 : 418-23
6) Graham JE, Snih
SA, Berges IM, Ray LA, Markides KS, Ottenbacher KJ.
Frailty and 10-year mortality in community-living Mexican
American older adults. Gerontology 2009; 55 : 644-51
7) Ensrud KE, Blackwell
TL, Redline S, Ancoli-Israel S, Paudel ML, Cawthon PM
et al. Sleep disturbances and frailty status in older
community-dwelling men. J Am Geriatr Soc 2009; 57 :
2085-93
8) Abellan van Kan
G, Rolland Y, Bergman H, Morley J.E, Kritchevsky S.B,
Vellas B. The I.A.N.A Task Force on frailty assessment
of older people in clinical practice. J Nutr Health
Aging 2008; 12 : 29-37
9) Hogan DB, MacKnight
C, Bergman H. Models, definitions and criteria of frailty.
Aging Clin Exp Res 2003; 15 (Suppl. 1): 1-29.
10) Kenneth Rockwood,
Xiaowei Song, Chris MacKnight, Howard Bergman, David
B. Hogan, Ian McDowell, and Arnold Mitnitski. A global
clinical measure of fitness and frailty in elderly people.
Can Med Assoc J 2005; 173: 489-95
11) Stuck AE, Siu
AL, Wieland GD, Adams J, Rubenstein LZ. Comprehensive
geriatric assessment: a meta-analysis of controlled
trials. Lancet 1993; 342: 1032-6.
12) Charlson ME,
Pompei P, Ales KL, MacKenzie CR. A new method of classifying
prognostic comorbidity in longitudinal studies: development
and validation. J Chron Dis 1987; 40:373-83.
13) Slaets JP: Vulnerability
in the elderly: frailty. Med Clin North Am 2006;
90(4):593-601.
14) Pel-Littel RE, Schuurmans MJ, Emmelot-Vonk MH, Verhaar
HJJ. Frailty: defining and measuring of a concept. J
Nutr Health Aging 2009; 13(4):390-394
15) Rockwood K, Mitnitski A. Frailty in relation to
the accumulation of deficits. J Gerontol Med Sci 2007;
62:722-727.
16) Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories
of disability in the last year of life. N Engl J Med
2010; 362:1173-1180.
17) Benyamini Y, Idler E, Leventhal H, Leventhal E.
Positive affect and function as influences on self-assessments
of health: Expanding our view beyond illness and disability.
J Gerontol B Psychol Sci Soc Sci 2000; 55:107-116.
18) Ostir G, Berges I, Smith P, Smith D, Rice J, Ottenbacher
K. Does change in functional performance affect quality
of life in persons with orthopaedic impairment? Soc
Indic Res 2006; 77:79-93.
19) Ricauda N, Tibaldi V, Leff B, Scarafiotti C, Marinello
R, Zanocchi M, Molaschi M. Substitutive "hospital
at home" versus inpatient care for elderly patients
with exacerbations of chronic obstructive pulmonary
disease: A prospective randomized, controlled trial.
JAGS 2008; 56:493-500.
20) Patrick DL, Erickson P. Health status and health
policy. Oxford Univ. Press; 1993.
21) Rejeski W, Mihalko S. Physical activity and quality
of life in older adults. J Gerontol A Biol Sci Med Sci
2001; 56(Spec No 2):23-3
22) Eklund K, Wilhelmson K. Outcomes of integrated and
coordinated interventions targeting frail elderly people:
a systematic review of randomised controlled trials.
Health Soc Care Com 2009; 17:447-458.
23) Fried L, Ferrucci L, Darer J, Williamson J, Anderson
G. Untangling the concepts of disability, frailty and
comorbidity: implications for improved targeting and
care. J Gerontol A Biol Sci Med Sci. 2004; 59(3):255-263.
24) Folstein, M.F., Folstein, S.E., McHugh, P.R. ""Mini-mental
state". A practical method for grading the cognitive
state of patients for the clinician". Journal of
psychiatric research 1975; 12 (3), 189-98.
25) El Okl MA. Prevalence of Alzheimer dementia and
other causes of dementia in Egyptian elderly. MD thesis
2002; Faculty of Medicine, Ain Shams University
26) Crum, R.M., Anthony, J.C., Bassett, S.S., Folstein,
M.F. Population-based norms for the Mini-Mental State
Examination by age and educational level. JAMA.1993;
12,269(18):2386-91
27) Sheikh, J.I. & Yesavage, J.A. Geriatric Depression
Scale (GDS): Recent evidence and development of a shorter
version. Clinical Gerontology 1986; A Guide to Assessment
and Intervention, 165-173, NY: The Hawarth Press.
28) Shehata, A.S., El-Banouby, M.H., Mortagy, A. Prevalence
of depression among Egyptian geriatric community. Master
thesis, 1998; Faculty of Medicine, Ain Shams University
29) Katz S, Ford AB, Moskowitz RW, Jackson BA and Jaffe
MW. Studies of illness in the aged. The index of ADL:
A standardized measure of biological and psychosocial
function. JAMA 1963; 21(9): 185:914-919.
30) Lawton MP and Brody EM . Assessment of older people:
Self-maintaining and instrumental activities of daily
living. The Gerontologist 1969; 9(3): 179-86.
31) Coons SJ, Alabdulmohsin SA, Draugalis JR, Hays RD
Reliability of an Arabic version of the RAND-36 Health
Survey and its equivalence to the US-English version.
Med Care.;1998 Mar;36(3):428-32.
32) Ware JE, Sherbourne CD. The MOS 36-Item short form
health survey (SF-36). Med Care 1992; 30 (6): 473-83
33) Hickey A, Barker M, McGee H, O'Boyle C. Measuring
health-related quality of life in older patient populations:
A review of current approaches. Pharmacoeconomics. 2005;23(10):971-93.
34) Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood
K. Validity and reliability of the Edmonton Frail Scale.
Age Ageing 2006;35:526-569.
35) Brodaty H, Moore CM. The clock drawing test for
dementia of the Alzheimer's type: a comparison of three
scoring methods in a memory disorders clinic. Int J
Geriatr Psychiatry 1997; 12: 619-27.
36) Podsiadlo D, Richardson S. The timed 'Up and Go':
a test of basic functional mobility for frail elderly
persons. J Am Geriatr Soc 1991; 39: 142-8.
37) Rockwood K, Fox RA, Stolee P, Robertson D, Beattie
BL. Frailty in elderly people: an evolving concept.
Can Med Assoc J 1994; 150: 489-95.
38) National Institutes of Health, National Heart, Lung,
and Blood Institute . Clinical Guidelines on the Identification,
Evaluation, and Treatment of Overweight and Obesity
in Adults. The Evidence Report. 1998. NIH Publication
No. 98-4083.
39) Folstein, M. F., Folstein, S. E., McHugh, P. R.,
& Fanjiang, G. Mini-Mental State Examination User's
guide 2001; Odessa, FL: Psychological Assessment Resources.
40) Hayes V., Morris J.,Wolfe C. & Morgan M. The
SF-36 health survey questionnaire: is it suitable for
use with older adults? Age and Ageing1995; 24, 1120-1125.
41) Brazier J.E., Walters S.J., Nicholl J.P. & Kohler
B.
Using the SF-36 and Euroqol on an elderly population.
Quality of Life Research 1996; 5, 195-204.
42) Gladman J.R.F. Assessing health status with the
SF-36. Age and Ageing 1998; 27, 3
43) Hickey A, Barker M, McGee H, O'Boyle C. Measuring
health-related quality of life in older patient populations:
A review of current approaches. Pharmacoeconomics. 2005;23(10):971-93.
44) Ensrud KE, Ewing SK, Taylor BC, Fink HA, Cawthon
PM, Stone KL, Hillier TA, Cauley JA, Hochberg MC, Rodondi
N, Tracy JK, Cummings SR. Comparison of 2 frailty indexes
for prediction of falls, disability, fractures, and
death in older women. Arch Intern Med 2008; 168:382-389.
45) Ravaglia G, Forti P, Lucicesare A, Pisacane N, Rietti
E, Patterson C. Development of an easy prognostic score
for frailty outcomes in the aged. Age Ageing 2008; 37:161-166.
46) Avila-Funes, J.A., Helmer, C., Amieva, H., Barberger-Gateau,
P., Le Goff, M., Ritchie, K., Portet, F., Carrière,
I., Tavernier, B., Gutiérrez-Robledo, L.M., and
Dartigues, J.F. Frailty among community-dwelling elderly
people in France: the three city study. J Gerontol Med
Sci 2008; 63A:1089-1096.
47) Masel MC, Graham JE, Reistetter TA, Markides KS,
Ottenbacher KJ: Frailty and health related quality of
life in older Mexican Americans. Health Qual Life Outcomes
2009; 7:70.
48) Kanauchi M, Kubo A, Kanauchi K, Saito Y. Frailty,
health-related quality of life and mental well-being
in older adults with cardiometabolic risk factors. Int
J Clin Pract 2008; 62:1447- 1451.
49) Puts MT, Shekary N, Widdershoven G, Heldens J, Lips
P, Deeg DJ. What does quality of life mean to older
frail and non-frail community-dwelling adults in the
Netherlands? Qual Life Res 2007; 16:263-277
50) Claudio Bilotta, Ann Bowling, Alessandra Casè,
Paola Nicolini, Sabrina Mauri, Manuela Castelli, and
Carlo Vergani. Dimensions and correlates of quality
of life according to frailty status: a cross-sectional
study on community-dwelling older adults referred to
an outpatient geriatric service in Italy. Health and
Quality of Life Outcomes 2010; 8:56
51) Guse LW, Masesar MA. Quality of life and successful
aging in long-term care: Perceptions of residents. Issues
Ment Health Nurs. 1999;20(6):527-39.
52) Smith KW, Avis NE, Assmann SF. Distinguishing between
quality of life and health status in quality of life
research: A meta-analysis. Quality of Life Research.
1999;8(5):447-59
53) Andrew, M.K., Mitnitski, A.B., & Rockwood, K.
Social vulnerability, frailty, and mortality in elderly
people. PLoSONE 2008; 3(5).
54) Rochat, S., Cumming, R.G., Blyth, F., Creasey, H.,
Handelsman, D., Le Couteur, D.G., Naganathan, V., Sambrook,
P.N., Seibel, M.J., and Waite, L. Frailty and use of
health and community services by community-dwelling
older men: the Concord Health and Ageing in Men Project.
Age Ageing 2010, 39:228-233.
55) Blaum CS, Xue QL, Michelon E, Semba RD, Fried LP.
The association between obesity and the frailty syndrome
in older women: The Women's Health and Aging Studies.
J Am Geriatr Soc 2005;53(6):927-934.
56) Newman AB, Gottdiener JS, Mcburnie MA, Hirsch CH,
Kop WJ, Tracy R, Walston JD, Fried LP. Cardiovascular
Health Study Research Group. Associations of subclinical
cardiovascular disease with frailty. J Gerontol A Biol
Sci Med Sci 2001;56(3):M158-M166
57) Burke GL, Arnold AM, Bild DE, Cushman M, Fried LP,
Newman A, Nunn C, Robbins J. CHS Collaborative Research
Group. Factors associated with healthy aging: The Cardiovascular
Health Study. J Am Geriatr Soc 2001;49(3):254-262.
58) Fried LP, Kronmal RA, Newman AB, Bild DE, Mittelmark
MB, Polak JF, Robbins JA, Gardin JM. Risk factors for
5- year mortality in older adults: The Cardiovascular
Health Study. JAMA 1998;279(8):585-592.
59) Woods NF, LaCroix AZ, Gray SL, Aragaki A, Cochrane
BB, Brunner RL, Masaki K, Murray A, Newman AB. Women's
Health Initiative. Frailty: Emergence and consequences
in women aged 65 and older in the Women's Health Initiative
Observational Study. J Am Geriatr Soc 2005;53(8):1321-1330
60) Studenski S, Hayes RP, Leibowitz RQ, Bode R, Lavery
L, Walston J, Duncan P, Perera S. Clinical Global Impression
of Change in Physical Frailty: Development of a measure
based on clinical judgment. J Am Geriatr Soc 2004; 52(9):1560-1566.
61) Walston J, McBurnie MA, Newman A, Tracy RP, Kop
WJ, Hirsch CH, Gottdiener J, Fried LP; Cardiovascular
Health Study. Frailty and activation of the inflammation
and coagulation systems with and without clinical comorbidities:
Results from the Cardiovascular Health Study. Arch Intern
Med 2002;162(20):2333-2341.
62) Newman AB, Gottdiener JS, Mcburnie MA, Hirsch CH,
Kop WJ, Tracy R, Walston JD, Fried LP. Associations
of subclinical cardiovascular disease with frailty.
J Gerontol A Biol Sci Med Sci 2001; 56:M158-M166.
|