|
Abstract
Introduction: Pressure Ulcer (PU) is a
localized injury to the skin and/or underlying
tissue. Malnutrition correlates with PU and is
one of the main factors for PU development. Mini
Nutritional Assessment (MNA) has been designed
and validated by previous workers to provide a
single, rapid assessment of nutritional status
in elderly patients, which classified patients
into normal nutritional status, at risk of malnutrition,
or malnourished.
Objectives: Investigate the relationship
between nutritional status and PU and the possibility
of using the MNA to predict pressure ulcer outcomes.
The main aim is to investigate the relationship
between nutritional status using MNA and PU in
elderly hospitalized patients at King Abdul-Aziz
Medical City in Riyadh (KAMC).
Methods: The study is a cross sectional
study using pre-post test which included thirty
five elderly patients newly diagnosed with PU
admitted at KAMC. Nutritional status and PU was
assessed at baseline and after two months at the
end. Anthropometric measurements were taken and
blood samples collected to analyze albumin, blood
urea nitrogen (BUN), creatinine, before and after
two months.
Results: The results showed that 88.6%
of PU patients were malnourished or at risk of
malnutrition at baseline using the MNA test, and
there was a reduction in the MNA score with the
severity of PU. The MNA score was significantly
increased at post study, and 54.3% of the subjects
were healed completely from PU at the end. The
results showed that all patients classified as
normal nutritional status were completely healed
from PU, 79% of at risk of malnutrition were completely
healed, while only 24% of malnourished were completely
healed. The result showed that there was a significant
negative correlation between MNA score and age.
There were significant positive correlations between
MNA score and BMI, CC, MAC and albumin at baseline.
Conclusion: To conclude, the results indicated
that the severity of PU in elderly subjects is
affected by nutritional status using MNA score.
Thus, optimizing diet may help in treating and
reducing the severity of PU in elderly subjects.
This should be an integral part of any PU management.
Key words: Mini Nutritional Assessment,
Pressure ulcer, Malnutrition, Elderly
|
- - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
Introduction
In recent years, there has been a sharp increase in
the number of older persons worldwide [1] and more older
people are alive nowadays than at any time in the past
[2]. The proportion of the population aged 60 and over,
is also growing each year. By the year 2025, the world
will host 1.2 billion people aged 60 and over and that
is expected to rise to 1.9 billion in 2050 [3]. The
same trend is also predicted in the Eastern Mediterranean
Region; while the proportion of the elderly population
to total population was 5.8 % in 2000 it is expected
to reach 8.7 % by the year 2025 and 15 % by 2050 [4].
The proportion of people who are 60 years of age and
older in the Saudi population is 5.2% [5]. The proportion
of elderly subjects is expected to increase to 8.6%
by 2025 and 18.6% by the year 2050 [6].
Pressure ulcer (PU) is a localized injury to the skin
and/or underlying tissue usually over a bony prominence,
as a result of pressure, or pressure in combination
with shear and/or friction [7]. The prevalence of multiple
illnesses among the elderly people is usually increasing.
Many workers predict that this could lead to a considerable
increase in PU [8].
PU occurs in both hospital and community settings, often
in the elderly and/or immobile people with severe acute
illness and in those with neurological deficits. An
increasing elderly population with growing number of
multiple illnesses is being seen in western society
[9].
Malnutrition correlates to PU. Patients with PU or who
are vulnerable to PU have a significantly lower energy
intake than other patients not suffering from PU [10-11].
Malnutrition is one of the well-known factors for PU
development in hospitals and nursing homes [12-13].
The Mini Nutritional Assessment (MNA) has recently been
designed and validated to provide a single, rapid assessment
of nutritional status in elderly patients in outpatient
clinics, hospitals, and nursing homes. It has been translated
into several languages and validated in many clinics
around the world [14]. The MNA provides a simple, noninvasive,
and well-validated nutrition screening tool that can
quickly and easily identify older adults who are at
risk of malnutrition. it is targeted at those living
in the community, long-term care facilities, or nursing
homes and those who require social services and those
coming to acute care units. The MNA has been used and
validated in all these above mentioned settings. In
both medical practice and clinical research, the reliability,
ease of use, and effectiveness of the MNA have made
it widely acceptable for nutrition screening and assessment
of elderly people [14-15]. The MNA has become a vital
component of comprehensive geriatric assessment [14].
In this study, the association between nutritional status
using the MNA and the severity of PU in elderly hospitalized
patients at King Abdul-Aziz Medical City (KAMC) in Riyadh
was studied. According to the best of our Knowledge,
we haven't found any published study investigate the
association between MNA score and the severity of PU.
The results will draw attention on the possibility of
using the MNA score to predict PU outcome.
Rationale and Objective
Nutritional status has been correlated with the
development and healing of PU. Thus, the association
between MNA and the severity of PU in elderly patients
would draw attention to the possibility of using the
MNA to predict PU outcome. Therefore, the main aim is
to investigate the relationship between MNA score and
PU in elderly hospitalized patients at KAMC in Riyadh.
Methodology
Study design and site
The study was a cross sectional study using pre post
test, in which nutritional status and PU were assessed
at admission (baseline) and after two months of including
the elderly patients newly diagnosed with PU, admitted
at KAMC in Riyadh, Kingdom of Saudi Arabia.
This study was approved from three scientific committees;
Deanship of postgraduate at King Saud University, King
Abdullah International Medical Research Center (KAIMRC),
and King Abdulaziz City for Science and Technology (KACST)
and was funded by KACST.
Study sample and objects
All elderly (>
60 years old) patients newly diagnosed with PU admitted
at geriatric unit and/or long term care units (Wards
22, 23, 24 and 25) at KAMC in Riyadh are included in
the study. Forty four newly admitted elderly patients
were the study sample for a period of ten months (from
May 2011 to March 2012) in which 9 patients passed away.
Thirty five patients continued in this study in which
15 subjects were female and 20 subjects were male and
their mean age was 79.2 years ± 11.3.
Stages
and healing of pressure ulcer
PU status was assessed at the next day of admission
by a thorough visual skin assessment conducted by wound
team with a large practice specializing in the diagnosis
and treatment of PU. Wounds team consists of a dermatologist,
plastic surgeon, wound care nurse and elderly care nurse.
On the basis of the skin assessment, wounds team recorded
the characteristics (including stage) of all PUs observed.
Patients were also categorized based on the presence
and stage of PU.
The PU was assessed using the staging system of National
Pressure Ulcer Advisory Panel (www.npuap.org) [7] at
baseline. This scale is used widely for clinical evaluation
of PU and it has been recommended to guide the assessment
of PU [7].
To assess the healing status of PU after two months
at the end of the study we didn't use the PU score to
measure the improvement of PU status but we used the
healing classification (completely healed and not completely
healed).
Nutritional status
Nutritional status of elderly PU patients was screened
and assessed at admission and after two months at the
end of the study at KAMC in Riyadh. Dietitians in KAMC
in Riyadh assess weight status for each individual to
determine weight history and significant weight loss
from usual body weight, assess ability to eat independently,
and assess adequacy of total food and fluid intake.
Mini Nutritional Assessment
(MNA)
Nutritional status of elderly patients was assessed
using the MNA. MNA were mostly filled in by watchers
of patients (relatives or hospital caregivers) and some
were done by the patients.
The MNA scale (0-30 points) consisting of 18 point-weighted
questions, is composed of anthropometric measurements,
global assessment, dietary questionnaires and subjective
assessment. The answers were given a maximum of 30 points.
Depending on the score of the test, elderly subjects
involved in the study were classified into the following
categories: well-nourished [MNA points 24-30], at risk
of malnutrition [MNA points 17-23.5], and malnourished
[MNA < 17 points] [16].
Anthropometric measurement
Measurements of weight and height were measured by the
nurses at time of admission and after two months at
the end of the study. Midarm circumference (MAC) and
Calf circumference (CC) were measured by the researcher
on the next day of admission and after two months at
the end of the study.
Measurements of weight (to the nearest 0.1 kg) and height
(to the nearest 0.1 cm) were made using a portable scale
and a portable stadiometer, respectively. Knee height
was used to estimate the stature of a person who could
not stand, or for a person with an obvious spinal curvature.
The following equation was used to estimate the stature
from knee height; Stature for elderly = [(2.02 knee
height) - (0.24 age)]. BMI was calculated by dividing
the weight in kilograms by the square of the stature
in meters (kg/m2). MAC was taken on the front of the
non-dominant upper arm by measuring the halfway distance
between the inferior aspect of the acromion and the
olecranon. MAC was measured to the nearest 0.1 cm using
a flexible non-elastic tape. CC was taken while the
elderly patient was laid supine, and the left knee and
ankle were bent to a 900 angle. CC measurement was taken
with an insertion measuring tape. The loop of the tape
is moved up and down the calf to locate the largest
diameter, and the measurement was recorded to the nearest
0.1cm [17].
Biochemical indicators
Blood samples were collected by nurses at 9 a.m. and
processed for serum albumin, urea nitrogen (BUN), and
creatinine. A total of 5 ml of blood was drawn from
each subject. Blood samples were then centrifuged at
3500 r.p.m for 10 minutes in a refrigerated centrifuge
to separate serum samples from the cells. Serum samples
were stored at 22° C in plastic tubes until analysis.
All samples were measured at central lab of KAMC in
Riyadh.
BUN concentration was measured by urease and creatinine
concentration was measured by kinetic alkaline pictrate
methods. Serum albumin was determined by the spectrophotometric
bromcresol green method. The following values were considered
normal: albumin >35g/L; BUN 3.0 to 7.0mmol/L; serum
creatinine 40 to 110µmol/L [18].
Nutritional Management for PU:
The nutritional status for elderly subjects with PU
was screen and assess at admission. They refer all individuals
with PUs to dietitians in KAMC in Riyadh for early assessment
and intervention of nutritional problems.
Dietitians in KAMC in Riyadh provide sufficient calories
(30 kcal to 40 kcal per kg of body weight per day or
Harris-Benedict times stress factor (1.2 for stage 1
and stage 2 ulcer, 1.5 for stage 3 and stage 4 PU).
They adjust calorie based on weight loss, weight gain,
or level of obesity. They provide adequate protein for
positive nitrogen balance of individuals with PU (1.2g
to1.5g of protein/kg bw/d (stage1 and stage 2 PU), 1.5g
to 2.0g of protein/kg bw/d (stage 3 and stage 4 PU)).
However the hospital does not use any standard nutritional
assessment specialized for elderly such as MNA, subjective
global nutritional assessment, or malnutrition universal
screening test to evaluate nutritional status for elderly
patients
Results
The mean body weight,
BMI, CC, and MAC were higher at post study compared
to baseline (Table 1). Albumin value at post study was
higher than at baseline (Table 1). The results show
that there were no statistical differences in the other
biochemical measurements. The mean of MNA score was
12.4. However, at post study, the mean of MNA score
was increased significantly to 15.8 (Table 1).
Table 1: Anthropometric, biochemical measurements,
and MNA score of subjects at baseline and post study
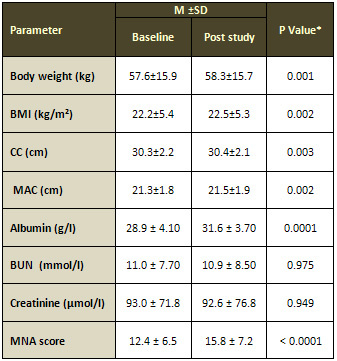
*Paired t test; P < 0.05 considered statistically
significant. M: mean. SD: standard deviation.
BMI: body mass index, CC: calf circumference, MAC: mid-arm
circumference, BUN: blood urea nitrogen, MNA: Mini Nutritional
Assessment.
The results show that 57.2% of elderly patients were
in stages 3 and 4 of PU at baseline, when they were
admitted to hospital. There were 54.3% healed completely
at the end of two months; 45.7% were not completely
healed (Table 2).
Table 2: Classification of pressure ulcer status
(healing status) of subjects at post study according
to pressure ulcer stage at baseline
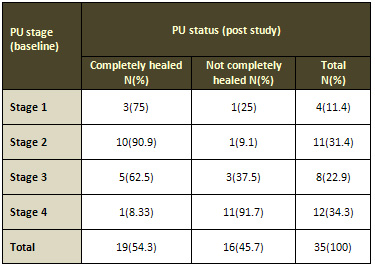
PU: Pressure Ulcer. N: number of cases. (%): percent.
Correlation between Pressure Ulcer Score and Mini
Nutritional Assessment Score at baseline
The results show that there is a significant negative
correlation between PU score and MNA score (Table 3).
Table 3: Correlation between Pressure Ulcer Score and
Mini Nutritional Assessment Score at baseline

R: Pearson correlation; P < 0.05 considered statistically
significant
Classification of nutritional status of subjects
Based on the MNA Score, it was found that 88.6% of the
patients were malnourished or at risk of malnutrition
at baseline. The percentage of the subjects classified
as malnourished at baseline decreased from 74.3% to
about 48.6% at post study (Table 4).
Table 4: Classification of nutritional status of
subjects at baseline and post study
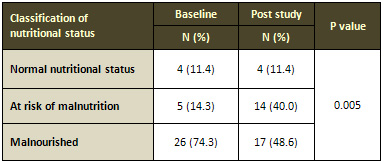
N: number of cases. (%): percent. *Paired t test; P
< 0.05 considered statistically significant.
Classification of nutritional status
The results show that most (69%) of malnourished patients
are at stage 4 and stage 3 of PU score at baseline (Table
5).
The results show that all patients classified as normal
nutritional status were healed, 79% of at risk of malnutrition
were healed and only 24% of malnourished subjects were
completely healed (Table 5).
Table 5: Classification of nutritional status in
relation to pressure ulcer stages at baseline
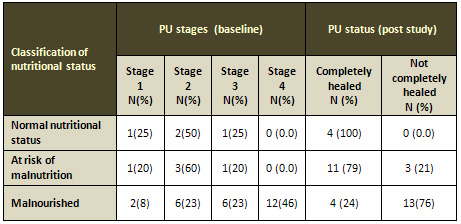
PU: Pressure Ulcer. N: number of cases. (%): percent.
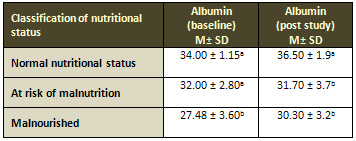
Mini nutritional assessment score and albumin
The results show that there was a reduction in the MNA
score and serum albumin with the severity of PU (Table
6). The results show that completely healed patients
had higher MNA score and albumin than not completely
healed (Table 7).
Table 6: Comparison between MNA score and PU stages
and between albumin and PU stages at baseline
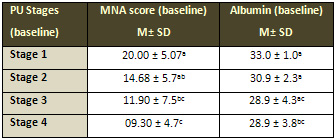
PU: Pressure Ulcer, MNA: Mini Nutritional Assessment.
M: mean. SD: standard deviation.
Means with different letter superscript are differ significantly.
Oneway Anova Test-Post Hoc Tests; P < 0.05 considered
statistically significant.
Table 7: Comparison between MNA score and PU status
and between albumin and PU stages at post study
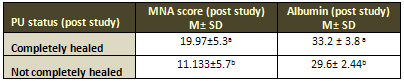
PU: Pressure Ulcer. MNA: Mini Nutritional Assessment.
M: mean. SD: standard deviation.
Means with different letter superscript are differ significantly.
Oneway Anova Test-Post Hoc Tests; P < 0.05 considered
statistically significant.
Classification of nutritional status and albumin
The results show that there was a reduction in the serum
albumin in all MNA groups and malnourished patients
had lower serum albumin level (Table 8).
Table 8: Classification of nutritional status in
relation to albumin at baseline
M: mean. SD: standard deviation.
Means with different letter superscript are differ significantly.
Oneway Anova Test-Post Hoc Tests; P < 0.05 considered
statistically significant.
Albumin and age
The results show that serum albumin had significant
negative correlation with advancing age and positive
correlation with BMI in PU elderly patients (Table 9).
Table 9: Correlation of albumin with age and BMI
at baseline
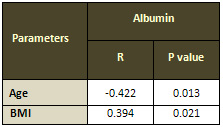
BMI: body mass index.
R :Pearson correlation; P < 0.05 considered statistically
significant.
Correlation between mini nutritional assessment score
and age, anthropometric and biochemical measurements
The results show that there were significant negative
correlations between MNA score and age and between MNA
score and BUN at baseline. There were significant positive
correlations between MNA score and BMI, CC, MAC and
albumin at baseline (Table 10). No significant correlation
was found between MNA score and creatinine.
Table 10: Correlation between mini nutritional assessment
score and various parameters at baseline
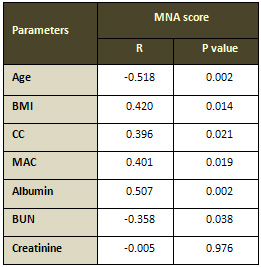
MNA: mini nutritional assessment. BMI: body mass index,
CC: calf circumference, MAC: mid-arm circumference,
BUN: blood urea nitrogen. R: Pearson correlation; P
< 0.05 considered statistically significant.
The correlation between MNA score and these parameters
were tested at post study and we found the same results
as at the baseline except BUN in which there is no significant
correlation found with MNA score at post study (data
not shown).
Discussion
and Conclusions
In the present study,
we investigate the nutritional status of elderly subjects
using the MNA score in PU patients at KAMC in Riyadh.
The results show that there was a reduction in the MNA
score with the severity of PU which may indicate that
PU is affected by nutritional status (Table 6). This
is accompanied by improvements in MNA score in which
34.6% of malnourished patients at baseline moved to
at risk of malnutrition at post study (Table 4). The
results show that all patients classified as normal
nutritional status were completely healed, 79% of at
risk of malnutrition were completely healed, and only
24% of malnourished were completely healed (Table 5).
This may indicate that nutritional intervention in addition
to other medical care has a role in improving PU status
of the elderly subjects at KAMC in Riyadh.
Wissing and Unosson (1999) showed that in free-living
elders with leg ulcers of any cause, (46%) and (3%)
were at risk of malnutrition and malnourished, respectively
[19]. Other studies show that more than 80% of PU elderly
patients were classified as at risk of malnutrition
or malnourished using MNA score [18-20]. This was consistent
with our study in which 88.6% of PU patients were malnourished
or at risk of malnutrition at baseline (Table 4). Because
malnutrition is one of the main factors of developing
PU, it is not a surprise in our study that about 88%
of the subjects were at risk of malnutrition or malnourished.
Hudgens et al (2004) show that subjects classified as
well nourished had a median stage 2 PU, whereas those
classified as at risk and malnourished had a median
stage 3 and stage 4, respectively [20]. In our study
the median stage of subjects classified as well nourished
or at risk of malnutrition is stage 2 PU, whereas those
classified as malnourished had a median stage 3. This
is accompanied by a significant negative correlation
between MNA score and PU score in our study. This may
be an indication that MNA test can be used to predict
the severity of PU.
Wissing et al (2001) show that MNA score increased over
time in healed PU subjects. This suggests that improving
MNA score is an indication of an enhanced wound healing
process[21]. This was consistent with our study in which
the MNA score was significantly increased at post study
compared to baseline (Table 1), and 54.3% of the subjects
were healed completely (Table 2).
Fifty percent to 70% of PU healed completely after nonsurgical
intervention has been applied [22]. Berlowitz and Wilking
(1990) show that 40% of PU patients completely healed
during a 6-week follow-up period [23]. In addition they
show that nutritional intervention and medical care
resulted in healing of 65% of stage II ulcers, 14% of
stage III ulcers, and 0% of stage IV ulcers over a 6-week
follow up period [23]. This was consistent with our
study (see Table 2).
Hudgens et al (2004) show that serum albumin was low
in all 3 MNA groups in PU patients who lived in an elders
nursing home [20]. In another study patients with MNA
>17 usually have a low albumin level [14].
This is consistent with our study in which serum albumin
was below normal range in all 3 MNA groups (Table 8).
Previous studies demonstrated that serum albumin levels
were lower in patients with PU compared with those without
PU [24], and was able to predict PU development with
adequate validity [25]. This is consistent with Bonnefoy
et al's (1995) study, that found that wound severity
can be influenced by albumin levels in patients with
PU [26]. In our study, the results show that there was
a reduction in the serum albumin level with the severity
of PU which indicates that PU may be affected by nutritional
status (Table 6). Furthermore the decrease in the level
of serum albumin could be due to inflammation that is
associated with PU. This is because albumin is one of
the negative acute phase proteins that decrease with
inflammation.
Serum albumin level has been traditionally considered
as a marker for PU healing [27] and also may be associated
with PU healing [28]. This is consistent with our study
in which the results show that completely healed patients
have higher serum albumin level than those not completely
healed (Table 7).
MNA score correlated with albumin level in elderly patients
[29-30]. In a residential home for the elderly, Salva
et al )1996( found that levels of serum albumin level
were highly correlated with the MNA score [31]. In our
study the MNA score correlates positively with serum
albumin level (Table 10).
The result shows that the MNA score correlated positively
with BMI, CC, and MAC (Table 10). This was consistent
with Langkamp Henken et al's (2005) study in which they
found that the MNA score correlated positively with
anthropometric measures including BMI, MAC and CC [18].
In a previous study show that levels of BMI were highly
correlated with the MNA score [31].
Shahin et al's (2010) study show a significant relationship
between the presence of PU in hospitals and undesired
weight loss[32], and weight loss were highly correlated
with the MNA score [31]. In our study, we found a significant
increase in BMI at post study (Table 1). This increase
in BMI may play a role in the healing process of PU.
Desneves et al (2005) found that PU patients who received
high caloric diet and supplementation of vitamins and
minerals noted a 2.5 fold greater improvement in healing
than PU patients who received regular diet [33]. A study
conducted by Wilson and his colleagues (2002) indicate
that individuals who consumed oral nutritional supplements
(protein, calories, fat, vitamins, minerals and/or amino
acids ) between meals accelerate the healing of PU [34].
In a study of 12 enterally fed patients with PU, the
group who received 1.8 g/kg of protein had a greater
decrease in PU surface area than the group receiving
1.2 g/kg of protein (the current recommended daily allowance)
[35]. This was consistent with our study (MNA questionnaires)
that there was increase in food intake (protein, vegetables
and fruits, and fluids). This was accompanied by improvement
of PU status in which 54.3 % were completely healed
and 45.7% were not completely healed (Table 2).
Using MNA, the subjects who consume at least one serving
of dairy products (such as milk, cheese, yoghurt) per
day and two or more serving of legumes or eggs per week
and meat, fish or poultry every day increased from 48.6%
at baseline to 62.9% at post study. This increase in
protein intake may have a role in the increase in albumin
level at post study and in the healing process of PU.
To conclude, the results indicate that the severity
of PU in elderly patients is affected by nutritional
status using MNA score. Diet may help in treating and
reducing the severity of PU in elderly subjects as shown
by the increase in protein intake and by the increase
in BMI and in the concentration of albumin level, which
is commonly used as indication of the nutritional status.
Recommendations
Serial assessments of elderly PU patients using the
MNA are recommended so that we can monitor the effectiveness
of nutrition interventions.
Performing nutritional screening and assessment is important,
but nutrition intervention should be adapted when patients
are identified as malnourished or at risk of malnutrition.
Nutrition assessments and interventions must be documented
so that the entire healthcare team is aware of the patient's
nutrition goals.
There was minimal information and limited studies in
the area of what nutritional intervention should be
implemented to reduce the risk of developing malnutrition
in PU patients, further studies are needed in this area.
References
1. Hafez G, Bagchi K, Mahaini R: Caring for the elderly:
a report on the status of care for the elderly in the
Eastern Mediterranean Region. EMHJ, July 2000; 6(4):
636-643.
2. McMurdo ME: A healthy old age: realistic or futile
goal? BMJ, 2000; 321(7269): 1149-1151.
3. World Population Prospects. The 2002 Revision, Highlights.
New York: United Nations Population Division, 2003;
(ESA/P/WP. 180).
4. WHO/EMR. Technical paper: Health care of the elderly
in the Eastern Mediterranean Region: Challenges and
Perspectives, 2003.
5. Population and housing characteristics in the Kingdom
of Saudi Arabia (KSA), Demographic survey 1428h (2007).
Central Department of Statistics and Information, Ministry
of Economy and Planning, KSA, 2007
6. World Population Prospects: The 2008 Revision, Highlights.
New York: United Nations Population Division.
7. Black J, Baharestani MM, Cuddigan J, Dorner B, Edsberg
L, Langemo D, Posthauer ME, Ratliff C, Taler G: National
Pressure Ulcer Advisory Panel's updated pressure ulcer
staging system. Adv Skin Wound Care. 2007; 20: 269-274.
8. Holm B, Mesch L, Ove H: The Australian Journal of
Advanced Nursing, Importance of nutrition for elderly
persons with pressure ulcers or a vulnerability for
pressure ulcers: a systematic literature review. 2007;
25: 77-84.
9. National Board of Health and Welfare: Current developments
in care of the elderly in Sweden (in Swedish).Stockholm.
2000.
10. Dambach B, Salle A, Marteau C, Mouzet J, Gahli A,
Faureau AM, Berrut G and Ritz P: Energy requirements
are not greater in elderly patients suffering from pressure
ulcers. Journal of American Geriatric Society, 2005;
53(3): 478-482.
11. Guenter P, Malyszek R, Zimmaro Bliss D, Steffe T,
Hara D, La Van F, Monterio D: Survey of nutritional
status in newly hospitalized patients with stage III
or stage IV pressure ulcers. Advanced Skin Wound Care,
2000; 13(4): 164-168.
12. Horn SD, Bender SA, Ferguson ML, Smout RJ, Bergstrom
N, Taler G, Cook AS, Sharkey SS, Voss AC: The national
pressure ulcer long-term care study: pressure ulcer
development in long-term care residents. J Am Geriatr
Soc, 2004; 52: 359-67.
13. Soini H, Routasalo P, Lagstrom H: Characteristics
of the mini-nutritional assessment in elderly home-care
patients. Eur J ClinNutr, 2004; 58: 64-70.
14. Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum
D, Lauque S, Albarede JL: The Mini Nutritional Assessment
(MNA) and its use in grading the nutritional state of
elderly patients. Nutrition., 1999; 15: 116-122.
15. Guigoz Y and Vellas B: Mini Nutritional Assessment
(MNA) Test to assess the nutritional status of the elderly:
The Mini Nutritional Assessment (MNA). Med Hyg, 1995;
53: 1965-1969.
16. Guigoz Y, Vellas B, Garry PJ. Mini nutritional assessment:
a practical assessment tool for grading the nutritional
state of elderly patients. Fact Res Gerontol 1994; suppl
2:15-59.
17. Chumlea WC, Roche AF, Mukherjee D eds: Nutritional
assessment of the elderly through anthropometry. (1987);
Ross Laboratories. Colombus, Ohio.
18. Langkamp-Henken B, Hudgens J, Stechmiller JK, Herrlinger-Garcia
KA: Mini nutritional assessment and screening scores
are associated with nutritional indicators in elderly
people with pressure ulcers. J Am Diet Assoc. 2005;105:
1590-1596.
19. Wissing U, Unosson M. The relationship between nutritional
status and physical activity, ulcer history and ulcer-related
problems in patients with leg and foot ulcers. Scand
J Caring Sci, 1999;13:123-128.
20. Hudgens J, Langkamp-Henken B, Stechmiller JK, Herrlinger-Garcia
KA, Nieves C Jr: Immune function is impaired with a
Mini Nutritional Assessment Score Indicative of Malnutrition
in Nursing Home Elders With Pressure Ulcers. Journal
of Parenteral and Enteral Nutrition, 2004. 28(6): 416-
422.
21. Wissing U, Ek AC, Unosson M: A follow-up study of
ulcer healing, nutrition, and life-situation in elderly
patients with leg ulcers. J Nutr Health Aging, 2001;
5: 37 - 42.
22. Kanj LF , Wilking SV , Phillips TJ: Pressure ulcers.
Journal of the American Academy of Dermatology, 1998;
38(4): 517 -538.
23. Berlowitz DR, Wilking SV: The short term outcome
of pressure sores. J Am Geriatr Soc, 1990; 38: 748-752.
24. Cordeiro MB, Antonelli EJ, da Cunha DF, Júnior
AA, Junior VR, Vannucchi H: Oxidative stress and acute-phase
response in patients with pressure sores. Nutrition,
2005;21: 901-907.
25. Anthony D, Reynolds T, Russell L: An investigation
into the use of serum albumin in pressure sore prediction.
J Adv Nurs, 2000; 32: 359-365.
26. Bonnefoy M, Coulon L, Bienvenu J, Boisson RC, Rys
L: Implication of cytokines in the aggravation of malnutrition
and hyper catabolism in elderly patients with severe
pressure sores. Age Ageing, 1995; 24 (1) : 37-42.
27. Gilmore SA, Robinson G, Posthauer ME, Raymond J:
Clinical indicators associated with unintentional weight
loss and pressure ulcers in elderly residents of nursing
facilities. J Am Diet Assoc, 1995; 95: 984-992.
28. Iizaka S, Sanada H, Matsui Y, Furue M, Tachibana
T, Nakayama T, Sugama J, Furuta K, Tachi M, Tokunaga
K, Miyachi Y: Serum albumin level is a limited nutritional
marker for predicting wound healing in patients with
pressure ulcer: two multicenter prospective cohort studies.
Clinical Nutrition, 2011; 30 : 738-745.
29. Gioulbasanis I, Georgoulias P, Vlachostergios PJ,
Baracos V, Ghosh S, Giannousi Z, Papandreou CN, Mavroudis
D, Georgoulias V: Mini Nutritional Assessment (MNA)
and biochemical markers of cachexia in metastatic lung
cancer patients: interrelations and associations with
prognosis. Lung cancer, 2011; 74(3): 516-520.
30. Duran Alert P, Mila Villarroel R, Formiga F, Virgili
Casas N, Vilarasau Farre C: Assessing risk screening
methods of malnutrition in geriatric patients: Mini
Nutritional Assessment (MNA) versus Geriatric Nutritional
Risk Index (GNRI). Nutr Hosp, 2012; 27(2): 590-598.
31. Salva A, Bolibar I, Munnoz M, Sacristan V: Results
of the "Mini Nutritional Assessment" (MNA)
in nursing home residents (abstract). J Am Geriatr Soc,
1996;44: 11.
32. Shahin ES, Meijers JM, Schols JM, Tannen A, Halfens
RJ, Dassen T: The relationship between malnutrition
parameters and pressure ulcers in hospitals and nursing
homes. Nutrition, 2010; 26: 886-889.
33. Desneves KJ, Todorovic BE, Cassar A, & Crowe
TC: Treatment with supplementary arginine, vitamin C
and zinc in patients with pressure ulcers: a randomised
controlled trial. Clinical Nutrition, 2005; 24(6): 979-987.
34. Wilson MM, Purushothaman R, Morley JE: Effect of
liquid dietary supplements on energy intake in the elderly.
The American Journal Of Clinical Nutrition, 2002; 75(5):
944-947.
35. Chernoff RS, Milton KY, Lipschitz DA: The effect
of a very high-protein liquid formula on decubitus ulcer
healing in long-term tube-fed institutionalized patients.
J Am Diet Assoc, 1990; 90: A-130.
|