|
Abstract
Background: Urinary tract infection is a very
common problem in general practice, but it is
more prominent in elderly patients and its average
prevalence is 25-40%. This is according to the
most recent studies. Perfect treatment of this
problem is very important because it is associated
with a lot of complications like pyelonephritis
and hypertension. This study was performed to
determine the benefits of good diagnosis and management,
depending on results of urine culture.
Methods: A retrospective study of homecare
residents was done between September 2010 to September
2011. We reviewed the medical records and files
of all patients.
132 patients of the total residents(614) had UTIs
within the period of study.
Results: One hundred and thirty two had
growth of microorganisms. Most of them were single
organism (80% of the growth is due to a single
organism), but about more than 50% were associated
with bacteria in the urine, usually more than
100,000 organisms per ml.
The most common causative organism was E.COLI
(57 patients) i.e 42.5% of total patients who
suffered of UTI.
Conclusions: Asymptomatic bacteriuria is
common in elderly patients, but it is more common
in women.
Pyuria is not a reliable predictor of bacteriuria.
Dementia, incontinence, catheterization, diabetes
mellitus & decreased mobility are risk factors
for developing UTIs.
Residential care residents often can't give reliable
histories.
Urinalysis and culture must be done for atypical
symptoms: - Change in behavior , Decrease in appetite
etc
Key words: Bacteriuria; long term care
patients, urine culture; sensitivity, Foley's
catheter, homecare
|
- - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
|
Abbreviations
APN:
acute pyelonephritis.
ASB: asymptomatic bacteriuria.
CKD: chronic kidney disease.
CRF: chronic renal failure.
CVA: cerebro vascular accident.
DM: diabetes mellitus.
EGFR: estimated glomerular filtration rate,
ESR: erythrocyte sedimentation rate.
ESRD: end-stage renal disease.
FC: Foley Catheter.
GFR: glomerular filtration rate.
GP: general practitioner.
HHCS: home healthcare service.
IM: intramuscular.
IV: intravenous.
NHS: National Health Service.
LUTI: lower urinary tract infection.
LRTI: lower respiratory tract infection.
RBC: red blood cells.
SPC: suprapubic catheter.
SPA: suprapubic aspiration.
UTI: Urinary tract infection.
WBC: white blood cell.
WHO: World Health Organization
|
Introduction
Urinary tract infection ( UTI) : By definition urinary
tract infection, or UTI, means any infection that can
affect any part of the urinary tract, which involves
:
1- Kidneys:
2- Ureters -- the tubes that take urine from each kidney
to the bladder.
3- Bladder.
4- Urethra -- the tube that empties urine from the bladder
to outside.
Or can be defined: is the presence of pathogenic bacteria
in the urine, urethra, bladder, kidneys or prostate.
The Public Health Laboratory Service uses the criteria
of 10 bacteria which are present in the urine for a
diagnosis(1)
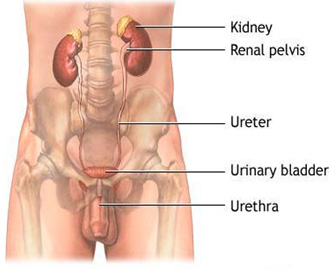
Figure 1: anatomical urinary tract system.
Urinary tract infection
(U T I) , & lower respiratory tract infection (LRTI)
are the most common problems in the elderly. Sometimes
there is misdiagnosis between those two problems, and
a lot of elderly patients are diagnosed as having LRTI
or UTI or even both but these diagnoses are not confirmed.
The most important cause for this problem is that many
elderly patients are unable to give a definite clinical
history suggestive of LRTI or UTI, because they are
often confused at the time of presentation. In such
conditions the correct diagnoses are the corner stone
in the management .This required a good clinical examination
and investigation, to differentiate between these two
problems.
Urinary tract infections are very common problems in
general practice in all age groups, but it is more common
in elderly people, with a prevalence of approximately
20% in women over 65 years old. Women have a greater
prevalence than men, but the trend to increase prevalence
with age in over 65 year olds is greater in men(2).
This may be contributed to by many factors:
1. Immunosuppression.
2. Underlying chronic medical illnesses like
DM,HTN.RF
3. Urinary and fecal incontinence.
4. Depressed mental state like dementia, delirium.
5. Associated use of devices such as urinary
catheters and nasogastric tubes.
6. Medications that suppress the immune system
or the central nervous system (polypharmacy).
7. Advanced age.
8. Factors that promote person-to-person transmission
such as crowding and sharing of meals(3).
9. Mechanical changes involving the bladder and
urethra, such as increased post void residual urine,
or that allow bacterial attachment .
10. Prostatic enlargement in men .
11. Decreased estrogen in postmenopausal women.
12. Not drinking enough fluids(4).
The diagnosis of UTI in adult patients depends on the
history and the physical examination. The most common
signs and symptoms of UTI are fever and/or chill, dysuria
(burning sensation of urine), pyuria, frequency, urgency,
Hematuria Colicky pain and incontinence. Cloudy urine,
foul or strong urine odor, pressure in the lower pelvis.
Diagnosis of UTI in confused elderly patients or those
who cannot express themselves is usually very difficult
, and sometimes may present in different ways; that
is the signs or symptoms are not related, like a patient
who presented with hallucination, disorientation, agitatation.
The most important challenge for physicians in long
term care setting is that under what conditions can
they give antibiotic as a treatment for possible UTI
in case of acute behavioral changes of demented patients
or those who cannot report classical symptoms of UTI
, which can help in making possible diagnosis.
In practice some demented elderly patients present with
acute behavioral changes like agitation; most of them
febrile. Those patients showed a significant improvement
when they were treated for UTI with antibiotic.
The perfect management of UTI in elderly patients is
very important, because it considers a serious infection
and carries a big chance for severe complications. UTI
in elderly patients usually differs significantly from
that which occurs in the general population, in its
etiology, clinical signs & symptoms, and treatment.
Definitions
1. Urinary tract infection means presence of
pathogenic bacteria in the urine, urethra, bladder,
kidneys, or prostate.
2. Recurrent UTI - Repeated episodes of infection
(three or more/year) by different causative microorganism.(5)
3. Relapse - Repeat UTI with the same strain
of microorganism within two weeks. This can be called
failure of the treatment.
4. Bacteriuria is presence of bacteria in urine
revealed by microscopy or by quantitative culture. Significant
Bacteriuria equal to or more than 105 cfu/ml of a single
bacterial species in a freshly voided specimen of urine.
a-women with symptomatic UTI >
102 cfu/ml .
b- men > 103
cfu/ml (if 80% of the growth is due to a single organism).(6)
5. Asymptomatic bacteriuria means presence of
bacteria in the urine with no signs or symptoms, discovered
microscopically in sample taken from patient's urine
or by urine culture.
6. Bacteraemia means presence of bacteria in
the blood and it is diagnosed by blood culture.
7. Empirical treatment of UTI is a treatment
based on clinical symptoms or signs unconfirmed by urine
culture.
8. Haematuria: it is presence of blood
in the urine either visible (macroscopic haematuria)
or invisible (microscopic haematuria) .
9. Catheterization: an indwelling catheter
is inserted through urethra or suprapubic temporarily
or permanently.
10. Short term catheter is an indwelling catheter
left in place for 1-7 days.(7)
11. Long term catheterization is an indwelling
catheter left in place for more than 4 weeks.
12. Pyuria : means number of white blood
cells (WBC)/ml equal or more than (104 cells ) per milliliter
of urine freshly voided.
13. Asymptomatic, abacteriuric patients: that
means Pyuria without bacteriuria and this is most likely
due to a foreign body, like urinary catheter, stones
or neoplasms of urinary tract, lower genital tract infection.
14. Dysuria : means painful urination,
or burning or stinging sensation and it is sometimes
described as difficulty of urination. This is the most
common symptom of lower UTI(8).
Background
Subject: Retrospective Study of urinary tract infection
( UTI) in geriatric patient under Homecare services for
the last year from 1st September 2010 until 1st September
2011.
Goals of the study
In this proposal we will try to focus / on urinary tract
infection to old age patients who live in their houses
under home care services.
1 To determine the prevalence of urinary tract
infection of the geriatric patients .
2 To identify the possible underlying risk factors
which may be related, to cause UTI.
3 To recognize the most common organism.
4 To determine the most appropriate antibiotic
for these organisms.
Epidemiology
PLACE: QATAR / DOHA/ HOMECARE
PATIENTS NUMBER: 614
DATE: 1stseptember 2010- 1st september2011
METHOD OF COLLECTION DATA: PATIENT FILES AND/ OR MEDICOM.
DURATION: 6 MONTHS
Collection data started at October 2011 retrospectively
For last year (1st September - 1st September 2011).
Total patients under home care for this period was614
patients, most of them were old age.
The ages were between 14-107 years.
67 patients aged between 14 -59 = 12.24%
547 patients aged between 60-107 = 87.76%
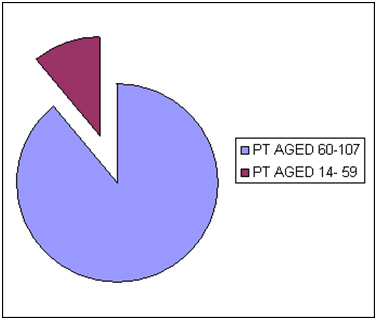
Figure 2: Distribution of patients according to age
Third paragraph explains the distribution of patients
according to their genders.
Total number of patients : ( 614)
Male patients : ( 212)
Female patients : (402 )
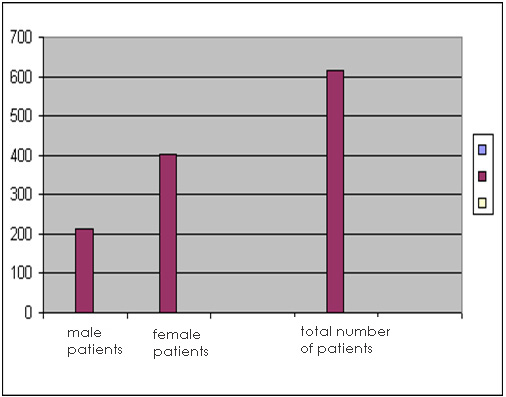
Figure 3: distributed patients according to gender
In this diagram we will try to show the distribution
of patients according to their nationalities.
|
QATARI |
541
|
| NON
QATARI |
73
|
| 1- PALESTINE |
20
|
| 2- BAHRAIN
|
10
|
| 3- PAKISTAN |
6
|
| 4- IRAN |
6
|
| 5- SUDAN |
5
|
| 6- YEMEN |
5
|
| 7- UAE |
4
|
| 8- JORDAN |
3
|
| 9- SOMALIA |
3
|
| 10- UK |
2
|
| 11- USA |
2
|
| 12- BANGLADESH |
2
|
| 13- PHILIPPINES |
2
|
| 14- CANADA |
1
|
| 15- SUDAN |
1
|
| 16- OMAN |
1
|
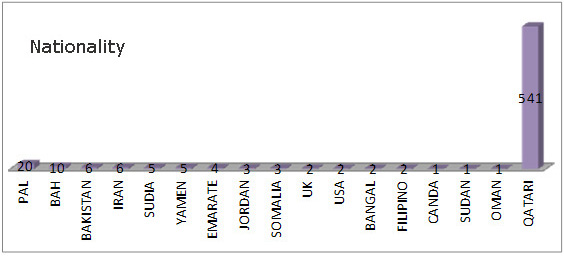
Figure 4: patients according to nationality
Methods
We traced electronic medical records and patients' files
during last year to collect these data. We depended
on result of urine culture and urine analysis.
Results
and Statistical Analysis
During data collection we found a lot of valuable things.
Here we will mention the most important findings :
A : None of total number of patients suffered from
UTI 131.
Two (2) patients were on intermittent catheter.
Three(3) patients were on condom catheter.
Five(5) patients were on suprapubic catheter.
Twenty nine(29) patients on Foley catheter.
Total catheterization patients had UTI ( 38 ).
This / means that 29% of total no. of UTI patients.
This means as we mentioned above, catheterization considered
as an important risk factor for UTI, and increases the
chance of infection.
All chronic catheter users have bacteriuria. Its treatment
does not improve mortality or morbidity but does increase
the risk of antibiotic-related side effects and the
development of infection with resistant organisms .(9)
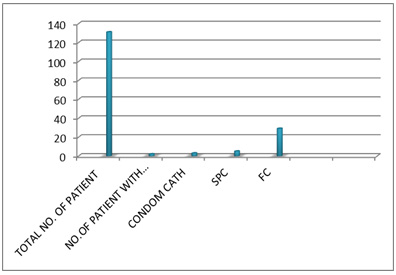
Figure 5: catheterization patients
B : Causative microorganism :
a- E coli , it was the most
common microorganism
(57 patients ) i.e 42.5% of total patients who suffered
from UTI .
b- 2nd common causative organisms
:
They were
1- pseudomonas aeruginosa.
2- klebseilla ssp.
3- enterococcus feacalis.
These three organisms affected 36 patients.
About 27.27% of UTI patients. (12) had all of them.
These microorganisms form about 70% of total patients
suffering from UTI in this study. This is supported by
A retrospective analysis of urine culture results issued
by the microbiology department, Teaching Hospital, Karapitiya(10)
The common etiological agents are Escherichia coli, Pseudomonas
spp., Proteus spp., Klebsiella spp. and Enterococcus spp.
c- Mixed growth : 16 urine
samples of patients showed mixed growth.
d- No growth : 7 urine samples
showed no micro organism had been found .
e- fungal infection especially
candida ssp plays a role in this problem
Candida ssp grows from 7 urine samples that had been taken
from patients. All of them females
f- the rest of causative
organisms varied (5 patients) acitinebacter buammanii,
Citrobacter koseri' & streptococcus feacalis , are
affected (2 patients) for everyone of them.
g- others : (3 patients)
other organism.
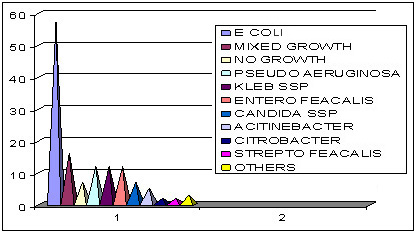
Figure 6: organism found in urine culture samples.
C : In the table below we choose more common causative
organisms of UTI. and sensitivity and resistance.
(E COLI , KLEPS ssp , ENTEROCCOCUS feacalis, PSEUDO MONAS
aeruginosa)
These organisms form around 70% of cases.
1st a- Ecoli (54 cases) 53 cases of them sensitive to
nitrofurantion, only one case is resistant.
28 cases (50% of cases) sensitive to septrin, 22 of cases
(40%) sensitive to Tazocin.
b- 32, 34, 38 cases, ie about (60% - 70% of cases) are
resistant to (cephalothin augmentin, ampicillin) respectively.
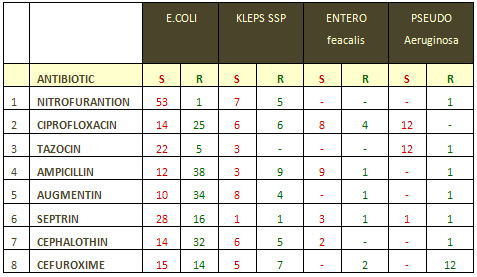
2nd (12 cases) of pseudomonas aeruginosa , 100% of them
are sensitive to Tazocin & ciprofloxacin .
3rd ( 12 cases) of enterococcus
feacalis , (8, 9 of them) are sensitive to ciprofloxacin
& ampicillin respectively .
4th (12 cases) of klepseilla
ssp, (6, 7, 8) are sensitive to ciprofloxacin Nitrofurantion
& augmentin respectively
D : UTIs associated with
chronic medical problems. 70 patients from those who
had UTI / suffered from DM for a long time. i e 53.43%
1- Diabetes mellitus is usually cited as increasing
the risk of infection all over the body
2- Patients with diabetes mellitus (DM) have an
increased risk of UTI, but data explains truly linking
a diabetic condition to infectious risk is still not enough
and needs more studies in future.
3- Uncontrolled Hyperglycemia appears to affect
the function of neutrophils with impairment of phagocytosis,
chemotaxis/migration as well as intracellularlysis of
organisms, and its affect on tissue perfusion leading
to peripheral vascular disease and microcirculatory abnormalities.
4- Diabetic peripheral neuropathy is a risk factor
for diabetic foot infection, Cellulitis and osteomyelitis,
5- Amputation in DM 15x > non-DM.
6- Patients with abnormal bladder function due
to neuropathy are at higher risk of UTI.
7- In US, 10% of all hospital discharges have a
DM diagnosis and therefore DM patients admitted more commonly
than non-diabetic patients(11).
8- Pneumonia and UTIs are the most common causes
of Diabetic ketoacidosis (DKA) and the hyperosmolar hyperglycemic
state (HHS) .
9- Data supports increased risk of UTI or pyelonephritis,
Candidal UTI, Candidal vulvovaginitis is still little
and needs more and more.
E : 71 patients developed MDRO i.e 54.19% .
The prevalence of resistance in organisms isolated from
UTI is well-recognized in old patients.
The mechanism of how organisms develop resistance to anti
microbials is not fully clear.
A few researchers tried to clarify and evaluate the importance
of potential factors contributing to resistance.
Some reports describe that resistance is derived from
older populations in long term care facility (LTCFs)(12),
But we still need more studies to answer many questions
like :
1. What is the prevalence of
resistance?
2. Is resistance associated with increasing age?
3. What are other associations of resistance in older
people ?
4. What is the appropriate management of UTI in older
People known or suspected to have symptomatic Infection
with a resistant organism?
5- Do older individuals with UTI with resistant organisms
have a poorer outcome than those with susceptible organisms?
6- How should bacterial resistance in UTI in older people
be defined?
(From: Resistant Pathogens in Urinary Tract
Infections) Lindsay E. Nicolle, MD JULY 2002-VOL. 50,
NO. 7, SUPPLEMENT)
F: 62 patients suffered
from recurrent UTI (relapse 10 cases) .
G : -in 53 patients WBC in blood increased
(10.700- 31.000) 4 cases showed decrease in no. of WBC
less than normal.
H : only 62 urine analyses had been done, 64.51
% of them support the diagnosis of UTI .
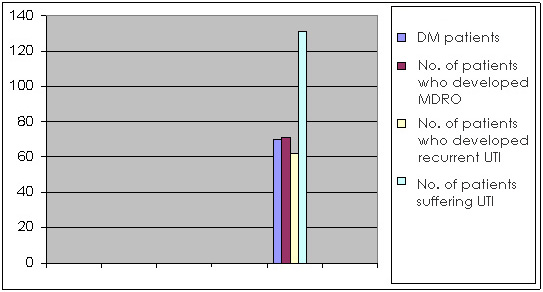
Figure 7: UTI associated
DM patients
I : This slide will show us percentage distribution
of males to females suffering from UTI:
1- 39 male patients suffered from UTI, this means
that 18.39% of total No. of male patients,
2- 92 female patients suffered UTI , this means
that 22,88 % of total No. of female patients.
*Women suffered with UTI more
than men; this fact has been proved by a lot of studies,
but the causes are still not clear
Figure 8: Males to females
patients
J : The most antibiotics
used in the treatment of UTI were as following:
|
1
|
ciprofloxacin
tab 500 mg oral bid 7- 14 days |
39
|
|
2
|
ceftriaxone
2 gr vial iv once daily 5-10 days |
27
|
|
3
|
tazocin 2.250- 4.5 vial iv gr tid 5-10 days |
23
|
|
4
|
cefuroxime
tab 250- 500 mg oral bid 7-14 days |
14
|
|
5
|
Azithromycin
250 -500 mg od oral 3-7 days |
10
|
|
6
|
Augmentin
tab 625mg oral bid 10- 14 days |
10
|
|
7
|
Meropenem
& Ertapenem 0,5-1 gr bid or tid
according to creatinine serum iv 7- 10 days |
7
|
|
8
|
Cefepime
1-2 gr iv bid 7- 10 days |
5
|
|
9
|
Nitrofurantoin tab 100mg bid oral 7 days |
4
|
|
10
|
Septrin
tab 960 mg bid oral 7-10 days |
4
|
|
11
|
Others |
7
|
|
12
|
No
treatment |
9
|
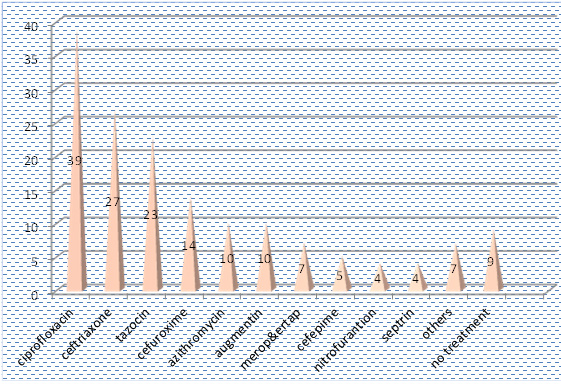
Figure 9: Antibiotics
most used in treatment of UTI
Summary
• The prevalence of resistant bacteria causing
urinary tract infection (UTI) from antimicrobials has
increased in the last decades especially in elderly
patients in the community.
• Patients in long-term care facilities, are more
liable to develop this problem than others .
• Resistant bacteria isolates include common uropathogens,
such as Escherichia coli and organisms with higher levels
of intrinsic resistance, such as Pseudomonas aeruginosa(13).
• It is essential to send urine specimens for culture
and susceptibility before starting antimicrobial therapy.
This gives the clinician a chance to select specific
antimicrobials for causative organisms and avoids empirical
therapy which is usually broad-spectrum antimicrobial.
• Antimicrobial therapy should be avoided unless
there is a clear clinical indication.
• Generally speaking asymptomatic bacteriuria should
not be treated with antimicrobials.
• In case empirical therapy is essential, before
isolated organisms recent antimicrobial therapy is the
drug of choice until result of culture is availiable
.
• Within ( 48- 72 hours) empiric therapy must be
reassessed.
• UTI is commonly over diagnosed and over treated
on the basis of nonspecific clinical signs and symptoms
.(14)
• Urinary tract infections are a very common presentation
in general practice in all age groups, with or without
catheters(15),
• The risk of infection will be increased if there
is any urological problem like abnormal structure of
the urinary tract
• Incomplete bladder emptying and urinary stasis
increases the incidence of bacteriuria especially with
increasing age and disability.(16)
• A high percentage of patients with indwelling
catheters (IDC) acquire bacteriuria each day even with
the application of best practice for insertion and care
of the catheter.
• In general, acute uncomplicated lower UTI is
usually due to one organism like Ecoli, or streptococcus
ssp ( 90-95%)(17)
• In patients with repeated infection, instrumentation
or recent hospitalization, MDRO must be suspected.(18)
• All patients with long-term catheters are bacteriuric
with urine samples and usually positive for two or more
organisms.
• Urinary tract infections (UTI) are the most common
infections acquired in hospitals and long-term care
facilities. Early studies estimate the incidence of
healthcare associated UTIs at around 2-3 patients per
100 admissions and this is supported by the more recently
published Plowman Report. (Plowman et al, 1999)(19)
• Recently a number of risk factors for healthcare
associated UTI have been established. The most important
predisposing factor for healthcare associated UTI is
the presence of an indwelling urethral catheter, and
chronic medical problem like DM (70 patients of 131)
as shownin our research .
• In elderly women (over 65 years of age), treatment
of asymptomatic bacteriuria does not reduce mortality
or significantly reduce symptomatic episodes. so no
need to treat these cases.
Prevention
1- Drink plenty of water is an important prevention
strategy.
2- Wipe from front to back.
3- Keep genital area clean and dry.
4- Do NOT drink fluids that irritate the bladder, like
alcohol and caffeine.
5- Drink cranberry juice or use cranberry tablets, but
NOT if you have a personal or family history of kidney
stones(20).
6- Use of low-dose antibiotics like Nitrofurantoin 100mg
once daily on a daily basis may be recommended to prevent
UTIs if patient gets frequent infections.
7- A good control of DM and treatment of other chronic
problems may play a role in decreased chance of getting
UTI .
8- Frequent emptying of the bladder and prevention of
congestion of urine is important to prevent growth.
9- Care giver must be able to pick up any changes in
patient behavior.
10- Early treatment of symptomatic patients with UTI
as soon as possible can be prevent more complications
.
References
PHLS (2001) Management of infection: Guidance for primary
care.
SCREENING FOR BACTERIURIA IN the elderly: A.Abyad, MD,
MPH, AGSF Director, Abyad Medical Center &
Middle-East Longevity Institute Abyad Medical Center
Tripoli-Lebanon
Uptodate subject UTI in elderly patients.
WEYTH.COM Urinary tract infection .
Scottish Intercollegiate Guidelines Network July 2006.
PHLS (2001) Management of infection: Guidance for primary
care.
Scottish Intercollegiate Guidelines Network July 2006.
Scottish Intercollegiate Guidelines Network July 2006.
Diagnosis and Management of Urinary Tract Infection
in Hospitalized Older People
Henry J. Woodford, MBBS, and James George, MBBS
Galle Medical Journal, Vol 13: No. 1, September 2008
.
Kidney infection in DM mahandeva santhakumar
Resistant Pathogens in Urinary Tract Infections) Lindsay
E. Nicolle, MD JULY 2002-VOL. 50, NO. 7, SUPPLEMENT
Resistant Pathogens in Urinary Tract Infections) Lindsay
E. Nicolle, MD JULY 2002-VOL. 50, NO. 7, SUPPLEMENT
Optimal management of urinary tract infections in older
people Clin Interv Aging. 2011; 6: 173-180.
Published online 2011 June 22. doi: 10.2147/CIA.S13423
Scottish Intercollegiate Guidelines Network July 2006.
Uptodate subject UTI in elderly patients .
Harison edition 16 2005 page 1718 .
Harison edition 16 2005 page1718 .
(Plowman et al, 1999) .
www.whfoods.org
|