|
Abstract
Background:
Community-acquired pneumonia (CAP) is an acute
disease that causes high mortality in the elderly,
and is a common cause of medical admission. Poor
prognostic factors of CAP include advancing age,
multiple co morbid illnesses, poor premorbid functional
status and severity of pneumonia
Objectives: A prospective
observational study was conducted to determine
the predictors of outcomes of (CAP) in Egyptian
older adults.
Subjects and Methods:
170 elderly patients; 72 males and 98 females
were recruited from Ain Shams University Hospitals,
diagnosed with CAP and required admission to the
hospital for treatment. Tools applied were: Comprehensive
Geriatric Assessment, Pneumonia Specific Risk
Index (PSI), CURB-65, The Charlson Comorbidity
Index (CCI),and Barthel Index (BI).
Results: CURB 65
and PSI showed significant differences for all
the outcomes (length of stay, ICU admission, ventilation
and mortality). Using the logistic regression
analysis, BI was found to be a significant predictor
for the length of hospital stay (P: .009, odd
ratio: 1.043, CI: 1.010 - 1.076) and ICU admission
(P: .003, odd ratio: .957, CI: .930 -.985). Regarding
the use of ventilator, age, functional condition
assessed by BI were significant predictors: (P:
.049, odd ratio: .932, CI: .869 - 1.000), (P:
.001, odd ratio: .950, CI: .921 - .980) respectively.
Regarding mortality, the three variables were
significant predictors for mortality; age: (P:
.001, odd ratio: 1.110, CI: 1.046 - 1.179), BI:
(P: .042, odd ratio: .968, CI: .939 -.999) and
CCI: (P: .019, odd ratio: .963, CI: .934 -.994).
Conclusion: PSI, CURB 65, BI and CCI were
significant predictors for the outcomes of CAP.
So inclusion of these assessment tools in the
evaluation of elderly patients suffering from
CAP can guide the physicians for the appropriate
management and levels of care needed for these
critical patients.
Key words:
Predictors of outcomes, elderly patients, pneumonia.
|
- - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
Introduction
There are three types of pneumonia in the elderly: community-acquired,
nursing home-acquired, and nosocomial pneumonia. Community-acquired
pneumonia refers to patients who live in their home;
these patients present more commonly than nursing home-acquired
patients because most elderly live in their own homes.
However, nursing home pneumonia patients are a population
deserving of special review
as they have different characteristics and tend to be
sicker than community pneumonia patients. [1]
Community-acquired pneumonia
(CAP) is an acute disease that causes high mortality
in the elderly; in-hospital mortality as high as 10%
is reported in patients aged 65 and older admitted to
the hospital with CAP, and many more die within a month
of discharge. Approximately 12% of survivors require
placement in a long-term care facility or rehabilitation
centre, and when long-term effects of CAP in elderly
patients have been investigated, there is a high risk
of subsequent mortality for several years. Additionally,
pneumonia is among the six-most-frequent discharge diagnoses
in patients with severe disability developed in the
previous year. Although short-term functional decline
has not been well studied in CAP, it has been well documented
in nursing-home residents. [2]
Community-acquired pneumonia
(CAP) is a common cause of medical admission. There
have been many studies on the association between pneumonia
and short-term mortality in older patients. Some may
use in-hospital mortality as the primary outcome, whereas
some may use 30-day mortality. Those in Europe showed
a wide range of in-hospital mortality from 6 to 26%
due to different inclusion and exclusion criteria. [3]
There are several international
guidelines on the prognostic indicators and management
of CAP. Poor prognostic factors included advancing age,
multiple co morbid illnesses and severity of pneumonia.
It was observed that premorbid functional status had
a strong bearing on the clinical outcomes of pneumonia.
Previous studies agreed that those with better premorbid
functional status had a shorter length of stay in hospital
and lower short-term and long-term case-fatality rates.
Poor functional status was also a risk factor for CAP
in immunocompetent old persons. [4], [5]
Old people with lower body weight
and recent weight loss had a greater risk of acquiring
CAP. It was logical to postulate that poor nutritional
status was associated with worse clinical outcomes.
[5]
The objective of this study
was to prospectively evaluate the effect of the severity
of the illness, the multiplicity of comorbidity and
functional status on the outcome of elderly patients
with CAP. It was hypothesized that these factors would
be important factors for the prognosis of CAP in the
elderly.
Subjects
and Methods
Design of study: Prospective observational
study.
Sample:
The study included 170 patients aged 60 or more; 72
males and 98 females diagnosed with CAP and were recruited
from Ain Shams University Hospitals over a period of
6 months.
The subjects included in the
study were diagnosed with CAP and required admission
to the hospital for treatment.
Inclusion criteria:
• Patients aged 60 or more.
• Diagnosed with new onset of abnormal infiltrates
on chest radiographs (interstitial shadowing, consolidative
changes or pleural effusion) and two of three clinical
features: fever (temperature > 37.8°C),
chest symptoms (shortness of breath, cough and increase
in sputum production or purulence) and abnormal chest
signs on physical examination (crepitations, bronchial
breathing or pleural effusion).
Exclusion criteria:
• Acute-care hospitalization for 72 hours or more
within the previous 15 days.
• Nursing-home residence.
• Non-oral feeding (nasogastric tube or percutaneous
gastrostomy).
• Final diagnosis other than pneumonia (acute heart
failure, pulmonary fibrosis, mesothelioma, bronchiolitis
obliterans, pleural effusion, patients with urinary
tract infection and patients with pulmonary infiltrates
due to pulmonary metastasis).
Clinical data recorded:
1. Informed oral consent.
2. Comprehensive Geriatric Assessment including
medical history and physical examination.
3. Laboratory and radiological data were collected
from patients' files to evaluate the severity of pneumonia
and to confirm their co morbidities.
All cases were treated with
the same plan of management according to the British
Thoracic Society Guidelines for the management of community
acquired pneumonia in adults: 2009 update [6]
Analyses:
From these data, four indices were calculated for studying
each patient in a complete and standardized way.
1. A validated Pneumonia
Specific Risk Index (PSI):
This index assigns a score based on 20 items that include
demographic factors, coexisting illnesses, physical
examination findings, and laboratory and radiographic
findings. Elderly patients are classified into four
risk classes; Class I (no predictor for mortality) was
not used in this analysis, outpatient care is recommended
for Class II patients (< 71 points), brief inpatient
observation for patients in Class III (71-90 points),
and traditional inpatient care for patients in Classes
IV (91-130 points) and V (>130 points). [7]
2. CURB-65:
Is a modification of the original British Thoracic Society
(BTS) rule and is designed to predict mortality in hospitalized
patients. [8]
The score is an acronym for each of the risk factors
measured. Each risk factor scores one point, for a maximum
score of 5:
• Confusion of new onset
• Urea greater than 7 mmol/l (19 mg/dL)
• Respiratory rate of 30 breaths per minute or
greater
• Blood pressure less than 90 mmHg systolic or
diastolic blood pressure 60 mmHg or less
• Age 65 or older
The risk of death at 30 days increases as the score
increases:
| 0-0.7% |
1-3.2% |
| 2-13.0% |
3-17.0% |
| 4-41.5% |
5-57.0% |
The CURB-65 is used as a means
of deciding the action that is needed to be taken for
that patient.
• 0-1: Treat as an outpatient.
• 2-3: Consider a short stay in hospital or watch
very closely as an outpatient.
• 4-5: Requires hospitalization with consideration
as to whether they need to be in the intensive care
unit.
3. The Charlson Comorbidity Index (CCI): [9]
The CCI predicts the ten-year mortality for a patient
who may have a range of comorbid conditions, such as
heart disease, AIDS, or cancer (a total of 22 conditions).
Each condition is assigned a score of 1, 2, 3, or 6,
depending on the risk of dying associated with each
one. Scores are summed to provide a total score to predict
mortality. Clinical conditions and associated scores
are as follows:
• 1 each: Myocardial infarct, congestive heart
failure, peripheral vascular disease, dementia, cerebrovascular
disease, chronic lung disease, connective tissue disease,
ulcer, chronic liver disease, diabetes.
• 2 each: Hemiplegia, moderate or severe kidney
disease, diabetes with end organ damage, tumor, leukemia,
lymphoma.
• 3 each: Moderate or severe liver disease.
• 6 each: Malignant tumor, metastasis, AIDS.
It scores from 1 to 6 for each of 18 specific medical
diagnoses, representing increasing levels of illness.
It has been shown to correlate with long-term survival
after acute medical illness.
The CCI can be used for prediction of 1-year survival,
prediction of 10-year survival and estimation of relative
risk of death.
In this study we used the predicted 1-year survival
rate that was calculated for all subjects through these
links:
http://tools.farmacologiaclinica.info/index.php?sid=37148&lang=en&loadsecurity=88
http://tools.farmacologiaclinica.info/index.php
4. Barthel Index (BI): [10]
Dependence in Activities of Daily Living (ADLs) 15 days
before the onset of illness was scored using the BI
which measures the capacity to perform 10 ADLs and obtains
a quantitative estimation of the patient's level of
dependence, scoring from 0 (totally dependent) to 100
(totally independent). This index has been proposed
as the standard for clinical and research purposes.
Clinical outcomes:
The patients were followed-up throughout their hospital
stay; several clinical outcomes were recorded including:
• Improvement and discharge.
• Length of stay in hospital.
• Admission to intensive care unit.
• Use of mechanical ventilation.
• In-hospital mortality.
Statistical Analysis:
All data were entered into the 21st version of SPSS
(Statistical Package of Social Science), and analyzed
using frequency and descriptive statistics to analyze
the study population. Frequency, percentage for all
qualitative variables and description of quantitative
variables in the form of mean (M) and standard deviation
(SD) were performed. Comparison of qualitative variables
was done using Chi-square test; it is a test that determines
the extent that a single observed series of proportions
differs from a theoretical or expected distribution
of proportions, or the extent that two or more series
proportions or frequencies differ from one another based
on the chi-square distribution. Multivariate logistic
regression analyses were used to adjust the influence
of the analyzed indices on outcomes. The regression
analysis included an examination of co-linearity by
using variance inflation factor. [11] Logistic regression
analysis was performed using the conditional forward
elimination procedure. Tests were two-tailed, and statistical
significance was determined at the 5% level.
Results
The study was conducted
on 170 older patients. Table 1 shows the demographic
and the clinical characteristics of the participants:
The mean age of the patients was 68.08 ± 5.8
(range: 60 - 88), 72 (42.4%) were males and 98 (57.6
%) were females; the minimum for CCI that predicts 1-year
survival rate was 11% and maximum was 92%, the minimum
for BI was 10/100 and maximum was 85/100; (mean 53.6,
±16.9), the mean duration of stay in hospital
was 6.3 ± 3.2, (range: 1 - 18 days), 131 patients
(77.1%) were CURB 65 II - III, while 39 patients (22.9%)
were CURB 65 IV - V. We found that 35 patients (20.6%)
were PSI II, 83 patients (48.8%) were PSI III, 33 patients
(19.4%) were PSI IV and 19 patients (11.2%) were PSI
V. 71 patients (41.8%) were admitted in ICU, 62 patients
(36.5%) were ventilated and 50 patients (29.4%) died.
Table 2 shows that regarding sex, there was no significant
difference between males and females in relation to
the outcomes except for mortality where sex was a significant
factor as mortality among females was 35 and males 15
(P: 0.035). While both indices that were used to determine
the severity of pneumonia (CURB 65 and PSI) showed significant
differences for all the outcomes (length of stay, ICU
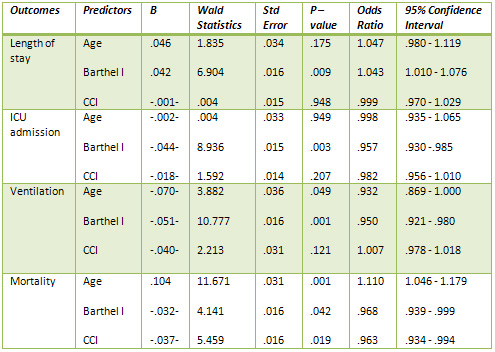
admission, ventilation and mortality). Table 3 shows
the logistic regression analysis and the patients' variables
used to predict the outcomes were; age, functional condition
assessed by BI and the severity of comorbidities assessed
by CCI. The table reveals that BI was a significant
predictor for the length of hospital stay (P: .009,
odd ratio: 1.043, CI: 1.010 - 1.076) and ICU admission
(P: .003, odd ratio: .957, CI: .930 -.985). Regarding
the use of ventilator, age, functional condition assessed
by BI were significant predictors: (P: .049, odd ratio:
.932, CI: .869 - 1.000), (P: .001, odd ratio: .950,
CI: .921 - .980) respectively, Regarding mortality,
the three variables were significant predictors for
mortality; age: (P: .001, odd ratio: 1.110, CI: 1.046
- 1.179), BI: (P: .042, odd ratio: .968, CI: .939 -.999)
and CCI: (P: .019, odd ratio: .963, CI: .934 -.994).
Table 1: Demography and characteristics of the study
sample:
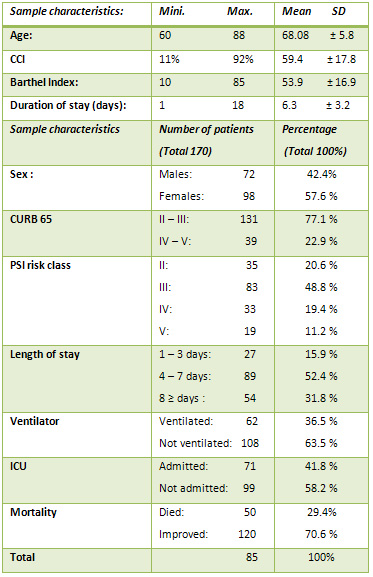
Table 2: Predictors of outcomes: analysis of patients'
qualitative variables:
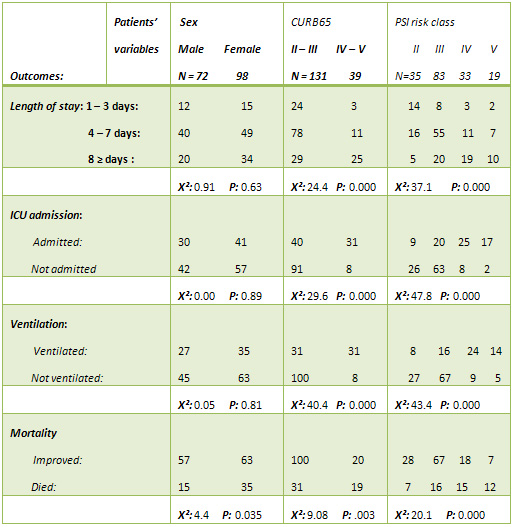
Table 3: Predictors of outcomes: analysis of patients'
quantitative variables: Results of the Logistic Regression
Analyses
Discussion
Our result showed that the mortality rate among the
participants was 29.4% and that advanced age was a significant
predictor for the use of ventilator and mortality and
female gender was a significant predictor for mortality
only while high scores in both indices that were used
to determine the severity of pneumonia (CURB 65 and
PSI) were predictors for all the outcomes (length of
stay, ICU admission, ventilation and mortality). Also
functional impairment was a predictor for all the outcomes
(length of stay, ICU admission, ventilation and mortality),
while severity of co morbidities was a predictor for
mortality only.
This was agreed with by El-Solh
et al., 2001 [12] who reported that the mortality rate
for older patients in hospital-based studies of community-acquired
pneumonia (CAP) were as high as 30%.
Also Kaplan et al., 2002 [13]
who studied 623,718 hospital admissions for community-acquired
pneumonia found that the overall mortality was 66,045
(10.6%) and added that mortality had doubled with age
from 7.8% in those aged 65-69 years to 15.4% in those
aged 90 and older.
The elevated rate of mortality
among elderly patients with CAP can be explained on
a physiological basis as the maximum function of the
respiratory system is reached at approximately the age
of 20-25 years. Thereafter, ageing is associated with
a progressive decrease in lung performance; however,
unless affected by disease, the respiratory system remains
capable of maintaining adequate gas exchange during
the entire life span. Physiological changes associated
with ageing have important consequences on the functional
reserve of older people, and their ability to cope with
the decrease in lung compliance and increase in airway
resistance associated with lower-respiratory-tract infection
(LRTI). Lower sensitivity of respiratory centres to
hypoxia or hypercapnia in older patients results in
a diminished ventilatory response in cases of acute
disease such as heart failure, infection, or aggravated
airway obstruction, and thus delays important clinical
symptoms and signs such as dyspnoea and tachypnoea,
which are important for diagnosis of pneumonia and appreciation
of the severity of the associated respiratory impairment.
[14]
Regarding the gender it was
found that female gender was a significant predictor
for mortality. While this was disagreed with Hon Ming
et al., 2011 [15], yet the higher number of females
than males in our study can explain this finding.
Our study revealed that the
severity of pneumonia assessed by CURB 65 and PSI showed
significant differences for all the outcomes (length
of stay, ICU admission, ventilation and mortality).
This was supported by Hon Ming
et al., 2011 [15] who studied 488 older patients aged
65 or above; mean age was 81.0 years (±7.9);
they were admitted for community-acquired pneumonia.
They found that CURB score and co morbidities were the
most powerful predictive factors of mortality of pneumonia.
Also Fine et al., 1997 [16]
stated that the PSI was a validated prediction rule
for prognosis that identified patients with pneumonia
at low risk for 30-day mortality and other adverse medical
outcomes. They added that the PSI was a good prognostic
score for CAP in adults.
According to Lim et al.,
2003 [17] there were two clinical prediction rules often
used to determine the prognosis; PSI and the CURB-65.
They stated that patients who were assessed to have
moderate and high risks of death were admitted to the
general ward and the intensive care unit (ICU), respectively,
therefore such prediction rules assisted in the appropriate
utilisation of limited hospital and ICU resources.
In the current study we found
that functional impairment was a predictor for all the
outcomes, and that the severity of co morbidities was
a significant predictor for mortality.
This was agreed with Kaplan et al., 2002 [13] who studied
623,718 hospital admissions for community-acquired pneumonia;
they found that mortality was higher in those with an
underlying illness defined by the Charlson-Deyo comorbidity
index (11.9% versus 7.6%, P < 0.006) using a univariate
analysis.
Also regarding functional status,
Mody et al., 2006 [18] agreed that those with better
premorbid functional status had a shorter length of
stay in hospital and also Jackson et al., 2009 [19]
found that poor functional status was a risk factor
for CAP in immunocompetent old persons.
And Torres et al., 2004 [20]
looked at the importance of functional assessment in
determining the outcome of CAP. Although they conducted
a small study of 99 patients aged 65 or older who had
community-acquired pneumonia, it showed that functional
status (using the BI) was an independent predictor for
short- and long-term mortality.
Also El-Solh et al., 2001 [21]
conducted studies used ADL in the construction of a
classification tree model for predicting outcome of
older patients with CAP requiring mechanical ventilation.
These studies suggest the importance of ADL ability
in predicting CAP outcome in other settings. Of the
analyzed indices, the only independent predictor for
short-term mortality was the BI. They found that functional
status measures had been shown to be important predictors
of hospital outcomes, and ADL dependence had repeatedly
appeared as an important predictor in nursing home pneumonia
studies.
Such information can be used
to assess the severity of pneumonia, particularly on
presentation and to be used to guide treatment and the
level of care, as well as allow predictions about prognosis.
In the elderly, decisions regarding the extent of investigations,
treatment (ie, intravenous versus oral antibiotics),
and whether intensive care management is appropriate,
need to be considered from the outset.
Implementation of these tools
for CAP patient's assessment leads to improved ability
to predict outcomes in elderly people with CAP, helping
clinicians with decisions such as whether to admit to
the hospital or to the ICU, and in-hospital interventions
for diminishing functional decline.
Conclusion
PSI, CURB 65, BI and CCI were significant predictors
for the outcomes of CAP. So evaluation of the severity
of pneumonia, functional status, and co morbidity of
the elderly patients suffering from CAP using these
tools can guide the physicians about the appropriate
management and levels of care needed for these critical
patients, accordingly. If patients are identified early
as being at high risk for complications, then they can
receive appropriate treatment in a timely manner, such
as hospitalization, ICU admission or ventilator support
if necessary.
References
1. Zalacain R, Torres A. Pneumonia in the elderly. Clinical
Pulmonary Medicine 2004; 11:210 -218.
2. Binder EF, Kruse RL, Sherman
AK et al. Predictors of short-term functional decline
in survivors of nursing home-acquired lower respiratory
tract infection. J Gerontol A Biol Sci Med Sci 2003;
58A:60-67.
3. Torres OH, Munoz J, Ruiz
D et al. Outcome predictors of pneumonia in elderly
patients: importance of functional assessment. J Am
Geriatr Soc 2004; 52:1603-9.
4. Mody L, Sun R, Bradley SF.
Assessment of pneumonia in older adults: effect of functional
status. J Am Geriatr Soc 2006; 54: 1062-1067.
5. Jackson ML, Nelson JC, Jackson
LA. Risk factors for community-acquired pneumonia in
immunocompetent seniors. J Am Geriatr Soc 2009; 57:
882-8.
6. Lim W S, Baudouin S V, George
R C, et al. Pneumonia Guidelines Committee of the BTS
Standards of Care Committee: Society Guidelines for
the management of community acquired pneumonia in adults,
Thorax 2009; 64: iii1-iii55.
7. Fine MJ, Auble TE, Yealy
DM et al. A prediction rule to identify low-risk patients
with community-acquired pneumonia. N Engl J Med 1997;
336:243-250.
8. Lim WS, van der Eerden MM,
Laing R, et al. Defining community acquired pneumonia
severity on presentation to hospital: an international
derivation and validation study. Thorax 2003; 58:377-382.
9. Charlson ME, Pompei P, Ales
KL et al. A new method of classifying prognostic comorbidity
in longitudinal studies: Development and validation.
J Chronic Dis 1987; 40:373-383.
10. Mahoney FI, Barthel DW.
Functional evaluation. The Barthel Index. Md State Med
J 1965; 14:61-65.
11. Kleinbaum DG, Kupper LL,
Muller KE. Applied Regression Analysis and Other Multivariable
Methods. Boston, MA: PWS-KENT Publishing Co., 1988.
12. El-Solh AA, Sikka P, Ramadan
F, Davies J. Etiology of severe pneumonia in the very
elderly. Am J Respir Crit Care Med 2001; 163: 645-51.
13. Kaplan V, Angus DC, Griffin
MF, et al. Hospitalized Community-acquired pneumonia
in the elderly: age and sex-related patterns of care
and outcome in the United States. Am J Respir Crit Care
Med 2002; 165: 766-772.
14. Janssens JP, Pache JC, Nicod
LP. Physiological changes in respiratory function associated
with ageing. Eur Respir J 1999; 13: 197-205.
15. Hon Ming MA, Wing Han Tang,
Jean Woo: Predictors of in-hospital mortality of older
patients admitted for community-acquired Pneumonia.
Age and Ageing 2011; 40: 736-741.
16. Fine MJ, Auble TE, Yealy
DM et al. A prediction rule to identify low-risk patients
with community-acquired pneumonia. N Engl J Med 1997;
336: 243-250.
17. Lim WS, van der Eerden MM,
Laing R, et al. Defining community acquired pneumonia
severity on presentation to hospital: an international
derivation and validation study. Thorax 2003; 58:377-82.
18. Mody L, Sun R, Bradley SF.
Assessment of pneumonia in older adults: effect of functional
status. J Am Geriatr Soc 2006; 54: 1062-1067.
19. Jackson ML, Nelson JC, Jackson
LA. Risk factors for community-acquired pneumonia in
immunocompetent seniors. J Am Geriatr Soc 2009; 57:
882-8.
20. Torres OH, Munoz J, Ruiz
D, et al. Outcome predictors of pneumonia in elderly
patients: importance of functional assessment. J Am
Geriatr Soc 2004; 52:1603-1609.
21. El-Solh AA, Sikka P, Ramadan
F. Outcome of older patients with severe pneumonia predicted
by recursive partitioning. J Am Geriatr Soc 2001; 49:1614-1621.
|