|
Abstract
Background: Cognitive impairment should be
accurately assessed in the elderly. The presence
of a valid Arabic version of the SLUMS Examination
would allow better diagnosis of cognitive impairment
as it considers different educational levels prevalent
in the Egyptian community.
Aim: To assess the reliability and validity
of the Arabic version of Saint-Louis-University-Mental-Status
(SLUMS) Examination for cognitive impairment and
to estimate the prevalence of cognitive impairment
among community dwelling Egyptian older adults.
Materials and methods: This study was conducted
in two phases: phase I, during which reliability
and validity of the Arabic version of SLUMS Examination
was assessed; then phase II, where the prevalence
of cognitive impairment among community
dwelling Egyptian elders was estimated using the
Arabic version of SLUMS Examination .
Results:
The phase I of the study was conducted on 90 elderly
group for testing validity and reliability of
the SLUMS tool. A statistically significant agreement
was evident between SLUMS Examination and Mini
Mental State Examination MMSE (Kappa 0. 826, P
<0.001). Sensitivity of SLUMS Examination was
94% (31/33) while Specificity was 96% (55/57).
SLUMS Examination was also found to be reliable
by test-retest. (McNemar P>0.05, Kappa 0.806
P<0.001). The internal consistency of the Arabic
version of SLUMS Examination on the main items
of cognitive function showed a Cronbach's alpha
of 0.723 with a significant item-to-item and item-to-total
correlation. The phase II of the study was conducted
on 284 elderly. 51.4% of them demonstrated mild
neuro-cognitive disorder and 5.6% were demented.
Age showed a significant relationship with cognitive
function level (P<0.001). Education level,
employment and depression showed significant differences
between elders with normal cognitive function
and the demented (P<0.001, P=0.003 and P <0.001
respectively).
Conclusion: The Arabic version of SLUMS-Examination
was found to be a valid and reliable screening
tool for cognitive impairment in elderly. Almost
half of the community dwelling Egyptian elderly
showed mild neuro-cognitive disorder and a minority
were demented. Older age, less education, unemployment
and evidence of depression were found to be significantly
associated with cognitive impairment. The Arabic
version of SLUMS-Examination should be included
in the routine assessment of cognitive impairment
in Egyptian elders.
Key words: Cognitive impairment, Egyptian
older adults, Arabic version of SLUMS-Examination
|
- - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
Introduction
Cognition is the process of thinking, learning, and
remembering. Cognitive impairment is not uncommon in
late life and may be due to the normal process of ageing
or associated with physical or mental disorders. [1]
It is characterized by memory disturbances, which occur
frequently among the elderly. [2]
The most common disease
causing cognitive impairment in the elderly is dementia.
There are many causes of dementia. Primary dementia
like Alzheimer's disease (AD) is the commonest cause
of dementia. Secondary causes of dementia include thyroid
disorders and deficiency of vitamin B12. Early detection
of dementia (primary or secondary) is of extreme importance
as treatment at an early stage yields encouraging results.
[1]
The prevalence of degenerative
dementias and other conditions associated with AD is
increasing due to the rapid ageing of the population.
The prevalence is below 1% among people aged 60-64 years,
but it shows an almost exponential increase with age.
In western countries, the prevalence ranges from 24%-33%
for people aged 85 years or older. It has been reported
that Chinese dementia patients make up 40% of all dementia
patients in the Asia-Pacific region and 25% of dementia
patients globally. [3] There are 6-7 million Chinese
people with dementia, with an incidence of 5-7% among
people over 65 years of age. Dementia patients experience
not only a serious decline in individual quality of
life but also impose a heavy economic burden on their
families and society. [4]
Dementia increases in prevalence
with age, with a doubling of prevalence every 5 years.
It is a progressive disease process affecting families,
caregivers, health and social care providers. Cognitive
impairment is an important part of the diagnostic criteria
for dementia. [5]
The discovery of the long preclinical
phase of AD of up to 7 years [6] led to enhanced interest
and research efforts in order to establish early diagnostic
indices of dementia. [7] In providing potential treatment
options for delaying or, ideally, preventing further
cognitive decline, the definition of high-risk populations
is of utmost importance. [8]
Mild cognitive impairment (MCI) is associated with an
increased risk of developing dementia: patients develop
dementia at a rate of 10-15% ? year compared with healthy
controls who develop dementia at a rate of 1-2% ? year.
[9]
However, data on the prevalence
and incidence of MCI as well as the conversion rate
to dementia varies greatly according to the different
definitional criteria applied. The rates of conversion
to dementia reported in the literature for example vary
from 1 to 25% / year. [10]
The prevalence of MCI increases
with age. The prevalence is 10% in those aged 70-79
years and 25% in those aged 80-89 years. [11]
Cognitive impairment is costly.
People with cognitive impairment report more than three
times as many hospital stays as individuals who are
hospitalized for some other condition. In 2009, AD and
related dementias alone were estimated to be the third
most expensive disease to treat in the United States.
The average Medicaid nursing facility expenditure per
state in 2010 for individuals with AD is estimated at
$647 millions, not including home- and community-based
care or prescription drug costs. [12]
More than 16 million people
in the United States are living with cognitive impairment.
[13] But the impact of cognitive impairment at the state
level is not well understood. Five states addressed
this shortcoming by assessing the impact of cognitive
impairment on their residents. This knowledge is vital
to developing or maintaining effective policies and
programs to address the needs of people living with
cognitive impairment in a state. Age is the greatest
risk factor for cognitive impairment, and as the Baby
Boomer generation passes age 65, the number of people
living with cognitive impairment is expected to jump
dramatically. An estimated 5.1 million Americans aged
65 years or older may currently have AD, the most well-known
form of cognitive impairment; this number may rise to
13.2 million by 2050. [14]
The Mini Mental State Examination
(MMSE) [15] is widely used in practice as a screening
tool for dementia. The MMSE has limitations, however,
especially with regard to its use in more educated patients
and as a screen for mild neuro-cognitive disorder. [16]
The Saint Louis University Mental Status Examination
(SLUMS) was developed to address this limitation. The
SLUMS is a 30-point, 11-item, clinician-administered
scale that is similar in format to the MMSE. [17] The
SLUMS, however, supplements the MMSE with enhanced tasks
corresponding to attention, numeric calculation, immediate
and delayed recall, animal naming, digit span, clock
drawing, figure recognition/size differentiation, and
immediate recall of facts from a paragraph. In particular,
the clock drawing test is designed to assess impairment
in executive function, one of the earliest forms of
cognition affected in mild neuro-cognitive disorder
and dementia. The SLUMS also eliminates some tasks that
appear on the MMSE, including repetition and construction.
By enhancing the SLUMS relative to the MMSE, it was
predicted that the SLUMS would be more sensitive and
specific than the MMSE, particularly for diagnosis of
mild neuro-cognitive disorder. [18]
Tariq et al., 2006 [19] found that the SLUMS and MMSE
both could be used as screening tools to detect dementia.
SLUMS also recognized a group of patients with mild
neuro-cognitive disorder, which the MMSE failed to recognize
as defined by DSM IV criteria. The sensitivity and specificity
appeared similar for both SLUMS and MMSE in detecting
dementia, but the SLUMS appeared to be possibly better
than the MMSE for differentiating mild neuro-cognitive
disorder from normal cognitive functioning.
So the aim of this study
was to assess the reliability and validity of the Arabic
version of SLUMS Examination for cognitive impairment
screening, as it adjusts for different levels of education
frequently encountered among the Egyptian population,
and to estimate the prevalence of cognitive impairment
among community dwelling Egyptian older adults using
this validated tool.
Participants
and Methods
This study was conducted in two phases: Phase
I; in which reliability and validity of the Arabic version
of SLUMS Examination was assessed, then Phase II; in
which the prevalence of cognitive impairment among community
dwelling Egyptian older adults was estimated using the
Arabic version of SLUMS Examination tool.
Phase I: Testing validity
and reliability of SLUMS:
Study setting and sample:
A cross-sectional study was conducted on 90 elder participants
(60 years old and above) (37 males and 53 females).
Elders were recruited from Egyptian social clubs in
Cairo city.
Data collection:
Socio-demographic data, namely age, gender, marital
status and education status were recorded for all participants
and an oral informed consent was obtained.
SLUMS Examination. [19]
Translation:
The SLUMS Examination was translated into Arabic language
and back translated into the original language, with
no significant difference between the original and the
back translated forms, but a few words were changed
to more convenient Arabic words adapted to the Egyptian
culture.
The SLUMS is a 30-point, 11-items,
clinician-administered scale that is similar in format
to the MMSE. [17] The SLUMS, however, supplements the
MMSE with enhanced tasks corresponding to attention,
numeric calculation, immediate and delayed recall, animal
naming, digit span, clock drawing, figure recognition/size
differentiation, and immediate recall of facts from
a paragraph. In particular, the clock drawing test is
designed to assess impairment in executive function,
one of the earliest forms of cognition affected in mild
neuro-cognitive disorder and dementia. [18]
The SLUMS is a one-page screening
test administered in 10 minutes to identify elderly
people with cognitive impairment. The total possible
score is 30. Interpretation of the score depends on
the level of education; High school education: Normal:
27-30; Mild neuro-cognitive disorder: 21-26; Dementia:
1-20. Less than high school education: Normal: 25-30;
Mild neuro-cognitive disorder: 20-24; Dementia: 1-19.
[19]
Mild neuro-cognitive disorder
is equivalent to MCI. MCI has been recently added as
the diagnosis of mild neuro-cognitive disorder in the
5th edition of The Diagnostic and Statistical Manual
of Mental Disorders (DSM-5) [20]
Validation:
All subjects were screened for the presence of cognitive
impairment by using the Arabic version of MMSE previously
validated. [21]
The Arabic version of SLUMS Examination was validated
in our study in reference to the MMSE that was administered
to all the participants to assess their cognitive function.
[15]
The MMSE comprises 30 questions with 10 devoted to orientation
(five for time and five for place). Three items required
registration of new information (repeating three words).
Five questions addressed attention and calculation.
Mental control questions required the patient to make
five serial subtractions of 7 from 100 or spell a word
backwards and three recall items (remembering the three
registration items). Eight items assessed language skills
(two naming items, repeating phrase, following a three-step
command, reading and following a written command and
writing a sentence), and one construction question (copying
a figure consisting of two overlapping pentagons).
According to the score of MMSE, the subjects were classified
into normal cognitive function, MCI and dementia (mild
to moderate and severe).
Reliability Testing
Test-retest reliability data were collected after an
average of 15 days as all 90 older adults were evaluated
again using the Arabic version of SLUMS Examination.
Phase II: Determination of
the prevalence of impaired cognitive function using
the Arabic SLUMS:
A cross-sectional study was
conducted to estimate the prevalence of cognitive impairment
in community dwelling Egyptian elder subjects.
Two hundred and 84 (284) old elders (60 years old and
above) 135 males and 149 females were recruited from
four Egyptian social clubs in Cairo city, over a period
of 3 months.
Data collection:
Socio-demographic data including age, gender, marital
status, living arrangement, employment and education
status were recorded for all participants and informed
consent was obtained.
Geriatric Depression Scale 15 items (GDS 15) was administered
to all participating elders. [22] as well as the Arabic
version of SLUMS-Examination.
Statistical Analysis:
Data collected was revised and introduced to a PC for
statistical management and analysis. Categorical data
is described as using frequency distribution (number
and percentage) while quantitative data is described
as using mean and standard deviation. One way ANOVA
was used to test differences in the tool categories
for continuous variables. Cronbach alpha was used to
test internal consistency of the Saint Louis items as
well as inter-items correlation. Paired t test was used
to test reliability and changes in the different items
of the Saint Louis instrument. McNemar Bowker and Kappa
statistics were used to test agreement between Saint
Louis and MMSE tools of cognitive impairment assessment.
Kendall tau-b was used to test correlation between ordinal
data. All p values were set at 0.05 and all statistical
manipulation and analyses were performed using the 15th
version of SPSS.
Results
The phase I of the study was conducted on 90 older adults
for testing validity and reliability of the SLUMS tool.
Table 1 shows the demographic characteristics of the
tested elders: their mean age was 67.3 ± 5.02
(range: 60 - 80). The sample included 37 (41.1%) males
and 53 (58.9%) females. Among the 90 elder participants;
42 (46.7%) were married, 38 (42.2%) widowed, 6 (6.7%)
divorced and 4 (4.4%) were single. 29 (32.2%) did not
complete their high school education while 61(67.8%)
terminated their high school education and some achieved
higher education.
Table 1: Patients' demographic characteristics in
Phase I:
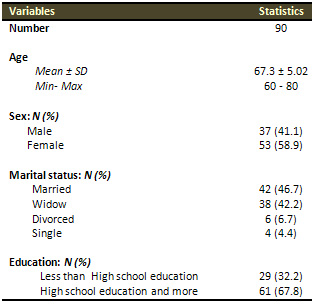
Table 2 shows significant agreement between the yield
of Saint-Louis-University-Mental-Status-SLUMS Examination
and Mini Mental State Examination MMSE (Kappa 0. 826,
P <0.001).
Compared to MMSE as a gold standard, sensitivity of
Saint-Louis-University-Mental-Status-SLUMS Examination
was 94% (31/33) while specificity was 96% (55/57).
Table 2: Correlation between SLUMS and MMSE:
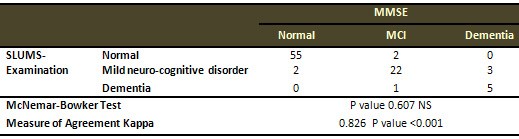
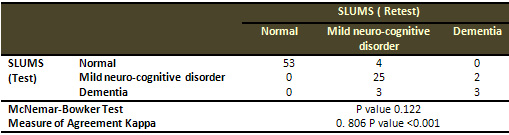
Table 3 shows significant reliability (Test-retest)
of Saint-Louis-University-Mental-Status-SLUMS Examination
(McNemar P>0.05, Kappa 0.806 P<0.001).
The internal consistency of the Arabic version of Saint-Louis-University-Mental-Status-SLUMS
Examination on the main items of cognitive function
showed a Cronbach's alpha of 0.723 with a significant
item-to-items and item-to-total correlation.
Table 3: Reliability (Test-retest) of Saint-Louis-University-Mental-Status-SLUMS-Examination:
The phase II of the study was conducted on 284 elders.
51.4 % of elders demonstrated mild neuro-cognitive disorder
and 5.6% were demented. Table 4 shows their demographic
characteristics: the mean age was 66.19 ± 4.56
(range: 60 - 82). The sample included 135 (47.5%) males
and 149 (52.5%) females. Among the investigated elders
144 (50.7%) were married, 111 (39.1%) widowed, 21 (7.4%)
divorced and 8 (2.8%) single. Thirty (30 = 10.6%) of
the interviewed elder were illiterates, 81 (28.5%) had
less than high school education and 173 (60.9%) achieved
a high school education and more.
Table
4: Patients' demographic characteristics in Phase II:
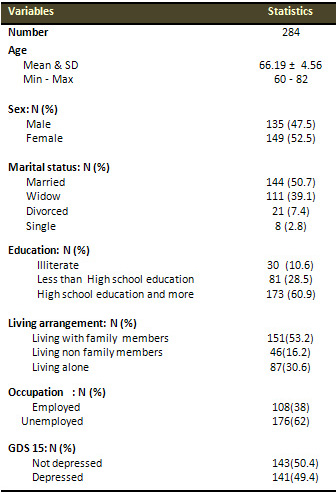
Figure (1) illustrates
the prevalence of cognitive impairment in the older
adults sample; 122 (43%) demonstrated normal cognitive
function, 146 (51.4%) showed mild neuro-cognitive disorder
and 16 (5.6%) had dementia.
Figure 1:
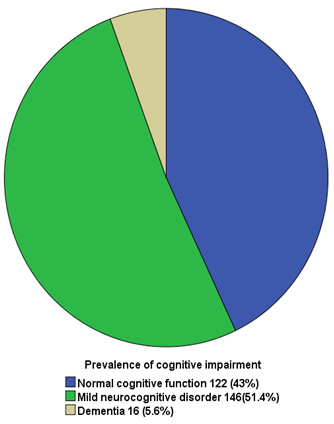
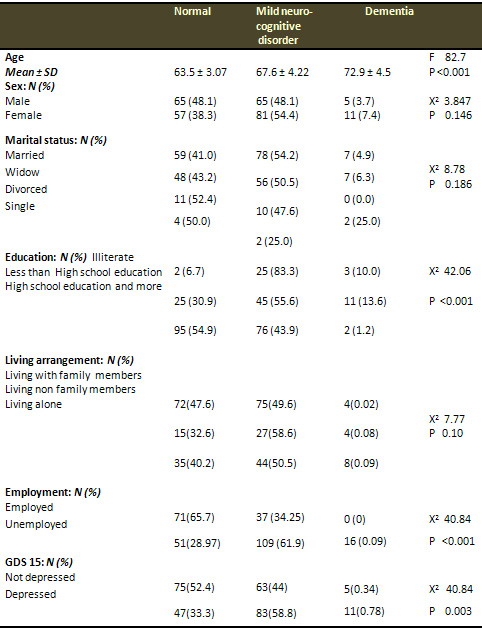
Table (5) shows the relationship
between patients' demographics and cognitive function.
Mean age of the normal cognitive function older adults
was 63.5 ± 3.07, while in demented cases was
72.9 ± 4.5, (P: <0.001). None of sex, marital
status and living arrangement showed a significant relationship
with cognitive function level, (P: 0. 146, P: 0.186,
P: 0.10), while education level, employment and depression
showed significant differences between older adults
with normal cognitive function and demented cases, (P
values: <0.001, 0.003 and <0.001 respectively).
Table 5: Relationship
between Patients demographic characteristics with Cognitive
function
Discussion
In the present study, the Arabic version of SLUMS Examination
demonstrated significant agreement with MMSE with high
sensitivity (94%) and specificity (96%), adequate test-retest
reliability and internal consistency.
The prevalence of mild neuro-cognitive
disorder in community dwelling Egyptian older adults
of the current study was 51.4% and dementia was 5.6%.
The prevalence of cognitive impairment in community
dwelling older adults varied in different studies depending
on characteristics of sample (e.g. rural versus urban
areas) and the tool used for screening of cognitive
impairment. For example the study conducted by Lee and
Shinkai, 2005 [23] in which they used the MMSE to estimate
the prevalence of cognitive impairment among Korean
people > 65 years of age, they found that the prevalence
was 17.0%.
A cross-sectional study was carried out by Deepak et
al., 2013 [24] between January 2010 and July 2010, in
urban and rural areas of Shimla district of Himachal
Pradesh in India. Four hundred elderly people were included
in the study. The prevalence of cognitive impairment
was found to be 3.5%. It was higher in rural (2.3%)
than in the urban population (1.3%).
Also Unverzagt et al., 2001 [25] conducted a study on
2212 community-dwelling African American residents of
Indianapolis, aged 65 and older and found that the overall
rate of cognitive impairment among community-dwelling
elderly was 23.4%.
Janice and Graham, 1997 [26] performed the Canadian
Study of Health and Aging that gathered population representation
information about elderly Canadians aged 65 and over
from 36 cities and surrounding areas in five regions.
In each region, the sample size was 1800 people in the
community and 250 people in institutions. Patients in
the community were screened for cognitive impairment
by means of the modified mini-mental state examination.
The prevalence of cognitive impairment no dementia [CIND]
was 16.8%, which was more than all types of dementia
combined (8.0%). They reported that the prevalence of
all types of cognitive impairment, including dementias,
increased with age.
Also we found that cognitive impairment increased significantly
with increasing age. This finding is in agreement with
Hardy and Higgins, 1992 [27] who examined the causes
of cognitive impairment and found that aging was the
predominant risk factor for MCI.
Again, Huang et al.,2008 [28] stated that previous studies
showed the prevalence of MCI to be higher in people
75 years of age and older than among those who were
younger than 75 years.
The age-cognitive function relationship is consistent
in both rural and urban areas as mentioned by Park et
al., 2013 [29] who stated that the mean score of MMSE
in both the urban and rural strata decreased with increasing
age.
Controversially, other results
revealed no significant relationship between age and
MCI. [30] Differences could be attributed to the selected
population or the tool used in cognitive function assessment.
As regards gender, although
7.4% of females were demented compared to only 3.7%
in males, this difference was not statistically significant.
Regarding this issue we disagreed with Greta et al.,
2005, [31] and with Park et al., 2013 [29] and with
Constanc et al., 2010 [32] as all of them had found
that female gender was significantly associated with
cognitive impairment. This could be explained by our
smaller sample size.
Also our study found that low
education was associated with cognitive impairment.
This was supported by Fratiglioni and Wang, 2007 [33]
who found that education was strongly related to the
risk of developing dementia. They added that this effect
was prominent in the Korean population compared with
that in other countries. They explained that this was
due to the generally lower education level among elderly
Koreans and the consequent lifelong lack of exposure
to stimulating environments and accessibility to health
services. Stewart et al., 2003 [34] added that lower
education level could hinder the early development of
brain function, and affect the absolute levels of cognitive
function.
Everson-Rose et al., 2003 [35] and Fratiglioni and Wang,
2007 [33] explained this as the intellectual challenges
might increase the brain reserve and delay development
of dementia.
Regarding the same issue, Park et al., 2013 [29] stated
that more years of schooling were associated with a
decreased probability of cognitive impairment, and Bosma
et al.,2003, [36] who conducted a 3-year follow-up study,
found that older persons with a lower educational level
experienced more decline in cognitive function; including
information processing speed, memory, and general cognitive
function according to the Mini-Mental State Examination,
compared to persons with a higher educational level.
As regards employment we found cognitive impairment
more prevalent in unemployed elders. Cognitive impairment
would interfere with employment and Occupation or employment
may act the same as education in improving the cognitive
function of the brain. Regarding this issue we agreed
with Park et al., 2013 [29] who found that employment
status was associated with a decreased probability of
cognitive impairment.
Regarding the relationship
between cognitive impairment and depression we found
that cognitive impairment was more prevalent in depressed
patients. So we agreed with Gao et al., 2012 [37] who
examined whether depression was a risk factor for onset
of dementia including Alzheimer's disease (AD), vascular
dementia (VD) and any dementia, and MCI by using a quantitative
meta-analysis of longitudinal studies. The quantitative
meta-analysis showed that depression was a major risk
factor for incidence of dementia (including AD, VD,
and any dementia) and MCI.
Again in the study of
Park et al., 2013 [29] they found that high GDS-15 scores
were significantly associated with increased cognitive
impairment.
Conclusion
The Arabic version of SLUMS-Examination was found to
be a valid and reliable screening tool for cognitive
impairment assessment. Almost half of the community
dwelling Egyptian elders showed mild neuro-cognitive
disorder and a minority were demented and are increasing
with age, less education, unemployment and presence
of depression. So, application of the Arabic version
of SLUMS-Examination in routine assessment of Egyptian
elders is mandatory.
References
1. Kua EH, Tan SL, Lee KS, et al. The National University
of Singapore NUH Memory Clinic. Singapore Medical Journal
1997; 38: 53.
2. Krishnaswamy S. Psychiatric problems among the elderly
in Malaysia. Med Malaysia 1997; 52: 222-24.
3. Anon (2009): There will be over 35 million patients
with elderly dementia in the globe.Available: http://www.ebiotrade.com.
Accessed 22 September 2010.
4. Zhou SN, Liu KB. The progress of gerontic dementia
in diagnosis and treatment. Chin Stroke, 2006; 10: 741-748.
5. Hofman A, Rocca W, Brayne C et al. The prevalence
of dementia in Europe: a collaborative study of 1980-1990
findings. Intl J Epidemiol 1991; 20: 736-48
6. Linn RT, Wolf PA, Bachman DL et al. The _preclinical
phase_ of probable Alzheimer's disease: A 13-year prospective
study of the Framingham cohort. Arch Neurol 1995;52:485-490.
7. Collie A, Maruff P. The neuropsychology of preclinical
Alzheimer's disease and mild cognitive impairment. Neuroscience
Biobehavioral Rev 2000;24:365-374.
8. Celsis P. Age-related cognitive decline, mild cognitive
impairment or preclinical Alzheimer's disease? Ann Med
2000;32:6-14.
9. Petersen RC, Stevens JC, Ganguli M, Tangalos EG.
Practice parameter: early detection of dementia: mild
cognitive impairment (an evidence-based review). Neurology
2001; 56:1133-1142.
10. Dawe B, Procter A. Concepts of mild memory impairment
in the elderly and their relationship to dementia -
a review. Int J Geriatric Psychiatry 1998;7:473-479.
11. Roberts RO, Geda YE, Knopman DS, et al. The Mayo
Clinic Study of Aging: design and sampling, participation,
baseline measures and sample characteristics. Neuroepidemiology.
2008;30 (1):58-69.
12. Alzheimer's Association. Characteristics, Costs
and Health Service Use for Medicare Beneficiaries with
a Dementia Diagnosis: Report 1: Medicare Current Beneficiary
Survey. Chicago: Alzheimer's Association; 2009.
13. Family Caregiver Alliance. Available at www.caregiver.org/caregiver/jsp/content_node.jsp?nodeid=438.
14. Herbert LE, Scherr PA, Bienias JL, Bennett DA, Evans
DA. Alzheimer's disease in the U.S. population: Prevalence
estimates using the 2000 census. Archives of Neurology
2003;60:1119-1122.
15. Folstein MF, Folstein SE, McHugh PR. Mini-Mental
State. A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res
1975; 12: 189-198.
16. Tombaugh TN, McIntyre NJ. The Mini-Mental State
Examination: A comprehensive review. J Am Geriatr Soc
1992; 40:922-935.
17. Morley JE, Tumosa N. Saint Louis University Mental
Status Examination (SLUMS). Aging Successfully, 2002;
XII (1): 4.
18. Royall DR, Cordes JA, Polk M. CLOX: An executive
clock drawing test. J Neurol Neurosurg Psychiatry 1998;
64:588-594.
19. Tariq SH, Tumosa N, Chibnall JT, Perry MH, Morley
JE. Comparison of the Saint Louis University mental
status examination and the mini-mental state examination
for detecting dementia and mild neurocognitive disorder--a
pilot study. Am J Geriatr Psychiatry. 2006 Nov; 14(11):900-10.
20. American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders, Fifth edition
(DSM-5). Arlington, VA: American Psychiatric Publishing;
2013
21. El-Okl MA, El Banouby MH , El Etrebi A. Prevalence
of Alzheimer dementia and other causes of dementia in
Egyptian elderly. MD Thesis, 2002; Faculty of Medicine,
Ain Shams University.
22. Beck AT, Ward CH, Mendelson M, et al. An inventory
for measuring depression. Arch. Of General Psychiat,
1961; 4: 561.
23. Lee Y, Shinkai S. Correlates of cognitive impairment
and depressive symptoms among older adults in Korea
and Japan. Int J Geriatr Psychiatry 20: 576-586.
24. Deepak Sharma, Salig Ram Mazta, Anupam Parashar.
Prevalence of cognitive impairment and related factors
among elderly: A population-based study. Journal of
Dr. NTR University of Health Sciences, 2013;2(3): 171-176.
25. Unverzagt F. W., Gao S., Baiyewu O., Ogunniyi A.
O., Gureje O., Perkins A., Emsley C. L., et al. Prevalence
of cognitive impairment Data from the Indianapolis Study
of Health and Aging Neurology November 13, 2001 vol.
57 no. 9 1655-1662.
26. Janice E Graham, Kenneth Rockwood, B Lynn Beattie,
Robin Eastwood, Serge Gauthier, Holly Tuokko, Ian McDowell.
Prevalence and severity of cognitive impairment with
and without dementia in an elderly population. The Lancet,
21 June 1997;Volume 349, Issue 9068, Pages 1793 - 1796,.
27. Hardy JA, Higgins GA. Alzheimer's disease: the amyloid
cascade hypothesis. Science, 1992; 256: 184-185.
28. Huang RY, Tang MN, Ma C, Guo YB, Han HY, et al.
The prevalence of mild cognitive impairment of residents
aged 60 years and over in the urban and rural areas
in Guangzhou. Chin J Nerv Ment Dis, 2008; 34: 533-537.
29. Park B, Park J, Jun JK. Cognitive Impairment, Depression,
Comorbidity of the Two and Associated Factors among
the Early Sixties in a Rural Korean Community. PLoS
ONE, 2013; 8(11): 10.
30. Yu H, Guo Z, Wang X. Exploration of high risk factors
in lifestyle for mild cognitive impairment in elderly
people. Progress in Modern Biomedicine, 2011; 10: 1885-1888.
31. Greta Rait, Astrid Fletcher, Liam Smeeth, Carol
Brayne, Susan Stirling, Maria Nunes, et al. Prevalence
of cognitive impairment: results from the MRC trial
of assessment and management of older people in the
community. Age and Ageing, 2005; 34: 242-248.
32. Constanc a Pau´, Oscar Ribeiro, Pedro Santos.
Cognitive impairment in old people living in the community.
Archives of Gerontology and Geriatrics, 2010; 51: 121-124.
33. Fratiglioni L, Wang HX. Brain reserve hypothesis
in dementia. J Alzheimers Dis, 2007; 12: 11-22.
34. Stewart R, Kim JM,
Shin IS, Yoon JS. Education and the association between
vascular risk factors and cognitive function: a cross-sectional
study in older Koreans with cognitive impairment. Int
Psychogeriatr, 2003; 15: 27-36.
35. Everson-Rose SA, Mendes de Leon CF, Bienias JL,
Wilson RS, Evans DA. Early life conditions and cognitive
functioning in later life. Am J Epidemiol, 2003; 158:
1083-1089.
36. Bosma H., van Boxtel M.P.J., Ponds R.W.H.M., Houx
P.J.H., Jolles J. Education and Age-Related Cognitive
Decline: The Contribution of Mental Workload. Educational
Gerontology, 2003; 29(2): 165-173.
37. Gao Y, Huang C, Zhao K, Ma L, Qiu X, Zhang L, Xiu
Y, et al. Depression as a risk factor for dementia and
mild cognitive impairment: a meta-analysis of longitudinal
studies. Int J Geriatr Psychiatry. 2012; 19: 10.
|