|
Abstract
Falls are increasing worldwide in an ageing population.
Commonly multi-factorial, falls in the elderly
need multidisciplinary teams to help their prevention
and recurrence. This was a retrospective study
analyzing falls and factors associated with them
over a 12 month period in the city of Sulaimani,
Kurdistan of Iraq. The results demonstrated well
established factors contributing to falls such
as age, female sex with multiple co-morbidities
and medications. More specifically to the Kurdistan
population the results related falls closer to
morning and prayer time or when washing. In addition,
those affected by falls are commonly living with
other family members. These results and studies
similar to this will allow the development of
specific interventions and services to help address
risk factors unique to a developing, Middle Eastern
population.
Key words: Falls,
Elderly, Prevention, Kurdistan
|
- - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
Introduction
The global elderly population
is increasing and as a consequence so is the burden
of non-communicable diseases.(1) Falls in the elderly
are a major cause for attending general practitioners
(GP) surgeries and emergency departments. Mechanical
(i.e. accidental falls) are uncommon among the elderly
population.(2) Falls in the elderly can be caused by
the interaction of intrinsic and extrinsic factors.
Significant examples include; patients with cognitive
impairment, those with foot deformities and medications,
especially anti-depressants.(3,4)
Falls in the elderly in developing
countries are increasing yet few studies exploring their
aetiology and prevention have been published.(5) In
Middle Eastern countries little is known about the prevalence
and features of falls. Data from an Iranian multicentre
study involving 2186 patients revealed that hip fracture
occurred in 26.2%. The study also identified that over
two thirds of falls occurred indoors.(6) The majority
of published studies on falls are from Western societies
and as a consequence the prevention strategies are based
on these populations. Sulaimany is a town in a newly
oil driven economically prosperous Kurdistan; an autonomous
region from the Iraqi central government since 1991.
The aim of this paper is to explore the risk factors
for falls specific to this population group. In gaining
a more detailed understanding of the causes of falls
in a developing population a more relevant prevention
strategy can be established instead of simply implementing
a Western guideline.
Methods
This retrospective study collected data on falls presenting
to hospital over a twelve month period. A proforma was
used to collect information. This included patient demographics
and factors associated with the fall (Appendix, Table
1). All patients admitted to the orthopedic, rheumatology
and emergency departments of the Sulaimany teaching
hospital who fell from at least their height level were
included in the twelve month window. Certain outcomes
were also measured such as severity and type of injury
or fracture. Admitting medical teams were directed to
fill out the pro forma.
Key points:
• Inclusion criteria; patient above the age of
60 who attended hospital due to a fall (defined as falling
from at least their own height).
• Data was collected using a pro forma questionnaire
(sample is attached) in the Sulaimany Accident and Emergency
department, medical and surgical wards.
Results
300 falls presented to Sulaimany hospital during the
twelve month window. 197 were female compared to 103
males. The mean age of fallers was between 70 and 74.
The majority occurred in the morning (72.6%) whilst
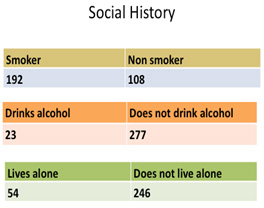
the patient was indoors (72.3%). Of the 300 falls 68.3%
had fallen before and 80.6% were on medications. 82%
lived with a partner or family and the remaining 18%
lived alone.
Discussion
Falls are multifactorial and as a result so too are
their prevention.(3) The risk factor for falls consequently
varies between populations and different cultural groups.
Identifying the risk factors for falls in elderly subpopulations
will allow the design of more specific interventions.
Cultural issues should be considered in falls prevention.
The daily routine, support network
and approach to healthcare will differ between subpopulations.
Many similarities are evident with the typical faller
in Western populations. Older females with multiple
medical co morbidities and medications account for the
majority of fallers. The differences however are apparent.
Fallers tend to live in families or with partners. In
Sulaimany the elderly remain living in family homes.
Notably there is an absence of residential or care homes.
Morning falls are more common (218 of the 300 falls).
Washing and toileting represent a major difficulty for
elderly patients which is emphasised by a lack of toileting
facilities. The toilet facilities are commonly a hole
at ground level. This is compared to western style toilets
which are raised at least two feet from the ground.
Toileting therefore requires a greater level of physical
effort and manoeuvrability. Facilities for washing in
Sulaimany are different from the UK. Waist level basins
are uncommon. Bending is required to reach for washing
taps which are commonly located on or near to the floor.
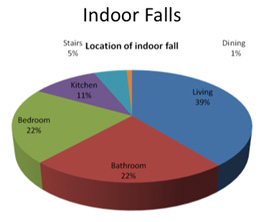
The majority of falls are also indoors. The reasons
behind this are most likely twofold. Firstly the housebound
elderly population has a higher disease burden and reduced
mobility. Secondly, certain indoor areas pose added
risks for falling. These areas can include the bathroom
but also other areas around a family house that elderly
populations in the UK do not encounter in a typical
retirement dwelling.
Morning Prayer is before sunrise.
Visual impairment and difficulty identifying the surroundings
are proven risk factors for falls. Reduced light at
this active time of day will compound these risks.(8)
Kurdish dress for ladies are a multi-layered long dress.
A high level of dexterity is required to perform the
activities of daily living in this traditional style
of clothing. The risk of falls is also increased due
to the clothing's potential interference with the environment.
Covering the whole body with such dresses for warmth
has proven to reduce exposure to sun light, hence reducing
Vitamin D and calcium metabolisms which contributes
to osteoporosis.(9)
This study has made some steps
to uncovering the many factors causing people to fall
in Kurdistan. Only patients who presented to hospital
were included. This represents a small number of total
fallers as those who fall in the community and do not
present to secondary care are being missed. By only
selecting patients who have sustained an injury it is
impossible to calculate the prevalence for all falls.
Similarly certain risk factors and characteristics are
potentially being underestimated. Further studies involving
community healthcare is needed to further improve the
knowledge of falls and associated risk factors. Such
research will also benefit Western fall prevention strategies
with many populations demonstrating an increasing Muslim
population.(10)
Recommendations from the
paper:
• Consider
falls risk specific for the Sulaimany population and
may be nationally for Kurdistan.
• Occupational
assistance to assess when fallers are at risk and aid
implementation of prevention strategies such as; help
during Morning Prayer, installing waist high basins
and ensuring areas are well lit before prayer.
• Adopting
a combined approach to falls management with other specialties
and allied health professionals.
• Harnessing
the presence of multiple family members within the faller's
home. Family intervention and education will be an important
tool in preventing falls in the Kurdistan community
• The local health
authority has to establish occupational assessment therapy
and introduce them to assess fallers' environment.
References
1. Kalache A, Keller I. The greying world: a challenge
for the twenty-first century. Sci Prog. 2000;83 ( Pt
1):33-54. PubMed PMID: 10800373
2. Cooper N, et al,(2009), ABC
of Geriatric Medicine, Chapter 4, 16-22, Wiley-Blackwell,
BMJ books.
3. Tinetti ME, Speechley M,
Ginter SF. Risk factors for falls among elderly persons
living in the community. N Engl J Med. 1988 Dec 29;319(26):1701-7.
PubMed PMID: 3205267.
4. Armstrong C, Swarbrick CM,
Pye SR, O'Neill TW. Occurrence and risk factors for
falls in rheumatoid arthritis. Ann Rheum Dis. 2005 Nov;64(11):1602-4.
Epub 2005 Apr 7. PubMed PMID: 15817660; PubMed Central
PMCID: PMC1755283.
5. Halil M, Ulger Z, Cankurtaran M, Shorbagi A, Yavuz
BB, Dede D, Ozkayar N, Ariogul S. Falls and the elderly:
is there any difference in the developing world? A cross-sectional
study from Turkey. Arch Gerontol Geriatr. 2006 Nov-Dec;43(3):351-9.
Epub 2006 Mar 7. PubMed PMID: 16522334.
6. Farid Abolhassania, Mohsen
Naghavib, Akbar Soltania,Bagher Larijania, Hamidreza
Tavakoli Shalmani Incidence and characteristics of falls
leading to hip fracture in Iranian population, Bone
39,2,408-413,2006
7. Campbell AJ, Robertson MC.
Implementation of multifactorial interventions for fall
and fracture prevention. Age Ageing. 2006 Sep;35 Suppl
2:ii60-ii64. Review. PubMed PMID: 16926208.
8. Figueiro MG, Gras LZ, Rea
MS, Plitnick B, Rea MS. Lighting for improving balance
in older adults with and without risk for falls. Age
Ageing. 2012 May;41(3):392-5. doi: 10.1093/ageing/afr166.
Epub 2011 Dec 13. PubMed PMID: 22166683; PubMed Central
PMCID: PMC3335369.
9. Gannagé-Yared MH,
Maalouf G, Khalife S, Challita S, Yaghi Y, Ziade N,
Chalfoun A, Norquist J, Chandler J. Prevalence and predictors
of vitamin D inadequacy amongst Lebanese osteoporotic
women. Br J Nutr. 2009 Feb;101(4):487-91. doi: 10.1017/S0007114508023404.
PubMed PMID: 18631414.
10. Dr Savita Katbamna, Mrs
Ruth Matthews, Leicester Nuffield Research Unit University
of Leicester, December 2006 Ageing & Ethnicity in
England, A Demographic Profile of BME Older People in
England, Age Concern.
|